

Urinary incontinence or incontinence is a common problem among premenopausal and menopausal women. Urinary incontinence belongs to the class of those problems that women, for obvious reasons, do not want to discuss even with their gynecologist.
Meanwhile, the problem is getting worse and significantly worsens the quality of life and the woman's ability to work. 45% of all cases of urinary incontinence are precisely stress incontinence, which means that hushing up the problem only delays its solution and exacerbates the entire pathological process. But with careful attention to your health and with the help of a competent doctor, you can eliminate the problem of urinary incontinence once and for all.
Stress urinary incontinence: causes
 There are several main types of urinary incontinence: stress, imperative, reflex, associated with neurogenic pathology of the bladder, bladder overflow incontinence and extraurethral incontinence, resulting from urogenital fistulas.
There are several main types of urinary incontinence: stress, imperative, reflex, associated with neurogenic pathology of the bladder, bladder overflow incontinence and extraurethral incontinence, resulting from urogenital fistulas.
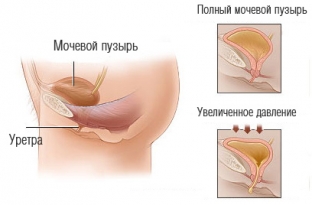
The most common is stress urinary incontinence, which is caused by an incorrect position of the proximal urethra. The muscular resistance of the urethra is insufficient and the pressure that arises in the abdominal cavity and the filled bladder is able to overcome it. That is why involuntary excretion of urine during stress incontinence occurs after physical activity, which provokes an increase in intra-abdominal pressure – when coughing, sneezing, while running and other physical activities.
Clinical presentation and stages of stress urinary incontinence
The clinical picture of stress urinary incontinence is different from other types of incontinence, since at rest a woman can control the urge to urinate relatively well, and involuntary excretion of urine occurs mainly against the background of physical exertion. In accordance with this, there are three degrees of clinical severity of stress urinary incontinence:
- at grade 1, urine output occurs with significant physical exertion: during coughing, sneezing, physical exertion and hard work;
- at grade 2, urine is excreted while walking, running, with a sharp rise or squats, and so on;
- The third degree is characterized by involuntary urination that occurs at rest, and not against the background of physical exertion.
Methods for diagnosing stress urinary incontinence
In the diagnosis of stress urinary incontinence, instrumental research methods play an important role: X-ray, urodynamic, ultrasound and magnetic resonance imaging. These methods help not only to visualize the state of the bladder and urinary tract, but also to assess their functional abilities directly during the act of urination. In addition, special fairly simple and affordable urological tests are used to diagnose stress urinary incontinence:
- levator test: assessment of the function of the levator ani muscle by inserting two fingers of the doctor into the vagina and contracting the pelvic muscles of the patient;
- bladder neck elevation test: when the posterior wall of the bladder is lifted with a finger inserted into the vagina, no urine should come out during coughing;
- cervicovesical elevation test: grasp the urethra with two fingers inserted into the vagina and bring the neck of the bladder closer to the symphysis, while no urine should be excreted during coughing;
- Q-tip-test: a special plastic stick with a cotton swab is inserted into the woman's urethra. During straining, the state of the urethra can be assessed by the degree of descent of the wand;
- stop test: this is a test that demonstrates the ability to voluntarily stop the act of urination, which indicates the functional viability of the female urinary system.
Stress urinary incontinence treatments
Treatment of stress urinary incontinence begins with conservative therapies. A woman is recommended special exercises that help strengthen the muscles of the pelvic floor and improve control over the act of urination. Of the medications, anticholinergics, antidepressants, calcium channel blockers, beta-adrenergic stimulants and dimethyl sulfoxide are widely used.
Conservative therapy is sufficient for the first degree of stress urinary incontinence, in other cases, surgical treatment is recommended. Vaginal and suprapubic surgeries, laparoscopic suspension and combined methods are performed, which aim to position the urethra in its physiological position and thus eliminate the problem of stress urinary incontinence.
Share:





Add a comment