

Today, the study of diseases caused by the Epstein-Barr virus is of interest to doctors of various profiles. This is due to the tropism of the virus to the immune system, as well as the importance of the virus in the occurrence of malignant neoplasms, in particular lymphomas.
Infectious mononucleosis – the most common pathology caused by the Epstein-Barr virus. It is also known as "kissing disease" due to the predominant route of infection.
This article on estet-portal.com provides detailed information on modern approaches to laboratory diagnosis of infectious mononucleosis.
The role of cytomegalovirus in the occurrence of infectious mononucleosis
Cytomegalovirus causes about 3% of cases of infectious mononucleosis. A feature of infectious mononucleosis caused by cytomegalovirus is the presence of prolonged febrile episodes, lymphadenopathy, and hepatitis. But at the same time, pharyngeal manifestations of the disease are absent in most cases.
Cytomegalovirus infection is especially dangerous during pregnancy: the risk of severe pathologies in the fetus is about 10%.
The possibility of cytomegalovirus to initiate the occurrence of infectious mononucleosis should be remembered when conducting laboratory diagnosis of the disease. Determination of the DNA of the virus by PCR confirms its role in the development of infectious mononucleosis.
Follow us on Telegram.
Changes in the CBC in infectious mononucleosis
Changes in the general blood test in infectious mononucleosis are quite characteristic. In the first days of the disease, leukopenia may be observed. Subsequently, it is replaced by leukocytosis with a predominance of mononuclear cells: in the general blood test, lymphocytes make up more than 50%. Thrombocytopenia and granulocytopenia are quite common in infectious mononucleosis. Against the background of liver damage, an increase in the levels of transaminases can be observed: ALT (alanine aminotransferase) and AST (aspartate aminotransferase).
See also: FDA warns increased risk of developing large cell lymphoma after breast implantation
Infectious mononucleosis: what are atypical mononuclear cells
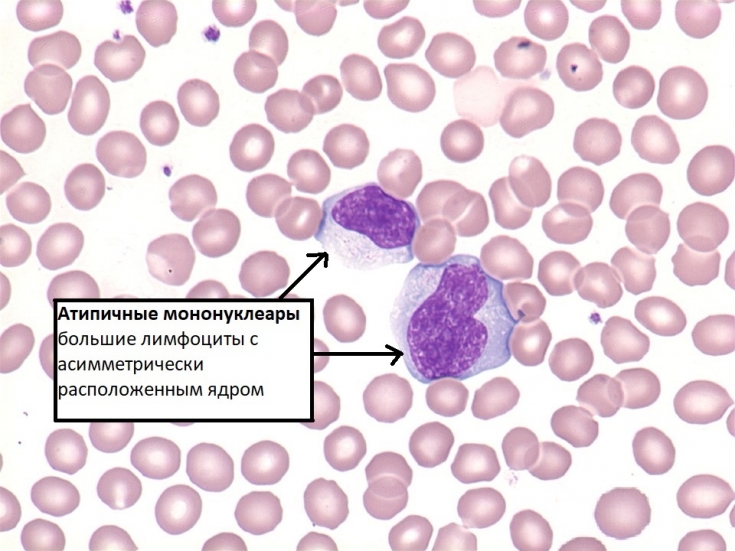
For patients with infectious mononucleosis, a very characteristic laboratory sign is the appearance of atypical mononuclear cells in the blood picture.
Atypical mononuclear cells – these are single-nuclear cells with a large nucleus, wide protoplasm and an enlightenment belt at the border of the nucleus and cytoplasm (the latter is not necessary). The cell nucleus is large and is located asymmetrically in the cell. Atypical mononuclear cells are young lymphocytes morphologically similar to monocytes. They are also known as "virocytes".
Atypical mononuclear cells can be present not only in infectious mononucleosis, but also in other viral diseases. But it is in the case of infectious mononucleosis that their number is more than 10%, which practically does not occur against the background of other viral infections and therefore is a diagnostic sign of infectious mononucleosis. In the blood picture, virocytes appear already on the 2nd-3rd day of the disease and can be observed for up to two months or more.
Insidious TORCH infections: what is the danger of toxoplasmosis during pregnancy
What is the serological diagnosis of infectious mononucleosis
Serological diagnosis of infectious mononucleosis consists of enzyme-linked immunosorbent assay (ELISA), which makes it possible to identify specific antibodies.
For the purpose of serological diagnosis of infectious mononucleosis, the enzyme immunoassay method is used.
Antibodies that are markers of infectious mononucleosis include:
1. anti-VCA Ig M (viral-capsid antigen from English – viral capsid antigen): are present in the blood from the very beginning of the disease in 100% of cases and are determined in the next 3 weeks in high titers. Anti-VCA IgM disappear by 1-6 months of illness. Their detection is specific both for the diagnosis of acute primary infection and its reactivation;
2. anti-VCA Ig G – can appear from 1-4 weeks of the disease, their number decreases with recovery. Their presence in most cases indicates the transferred infectious mononucleosis. An increase in titer by 4 or more times in dynamics indicates an acute infectious process.
3. anti-EBNA Ig G (Epstein–Barr nuclear antigen from English – nuclear antigen of the Epstein-Barr virus) – are identified the latest (4-6 months after the onset of the disease) and can persist for many years and even for life.
4. anti-EBV EA-D IgG (early D antigen – early D antigens) – are antibodies to the D-component of the protein required for virus replication. Characteristic of acute primary infection, appear in the first two weeks of the disease and quickly disappear with recovery. An increase in anti-EBV EA-D IgG titer indicates reactivation of the infection.
PCR can also be used to determine the etiology of infectious mononucleosis. The identification of Epstein-Barr virus DNA in blood and mucosal scrapings confirms its role in the development of the disease. The determination of heterophilic antibodies is practically not used nowadays due to technical difficulties and low specificity of the assays.
Thank you for staying with estet-portal.com. Read other interesting articles in the Infectious Diseases section. You may also be interested in: Why is it important to diagnose ring-shaped inflammatory skin lesions.
Share:





Add a comment