
Glucagonoma − neuroendocrine tumor of the pancreasislet alpha-2 cells. In 75-80% of cases, glucagonoma develops in a malignant form, of which metastases are found in 50% of cases.
The tumor is characterized by overproduction of glucagon. Clinically manifested by weight loss, diabetes mellitus, hypoaminoacidemia, normochromic and normocytic anemia, necrolytic erythema migrans, pulmonary embolism.
Modern methods of diagnosis and treatment of glucagonoma are presented to your attention in the article estet-portal.com.
The physiological role of glucagon in the body
Glucagon is a peptide hormone produced by the alpha-2 cells of the pancreas and, to a lesser extent, – diffuse neuroendocrine system (APUD-system) in the mucous membrane of the stomach and duodenum.
Glucagon is secreted under the influence of various factors. The most important of these is the reduction of blood glucose concentration. Acetylcholine and catecholamines increase serum levels of glucagon and somatostatin; serotonin reduces their content.
Glucagon functions:
1. activation of glycogenolysis with simultaneous inhibition of glycolysis and activation of gluconeogenesis;
2. stimulation of lipolysis and secretion of catecholamines;
3. inhibition of the secretory activity of the stomach, pancreas and motility of the gastrointestinal tract;
4. stimulation of urinary excretion of water, phosphates, sodium, calcium and magnesium ions.
Follow us on Telegram
Pathophysiology of glucagon in pancreatic tumor
Hyperglycemia associated with a pancreatic tumor is a consequence of the glycogenolytic and gluconeogenic effects of glucagon.
• Diabetes mellitus occurs in patients with glucagonoma due to an imbalance between the production of insulin and glucagon.
• Weight loss of 5-15 kg is associated with increased protein catabolism under the action of glucagon. It is likely that this mechanism is also responsible for the anemia and hypoaminoacidemia observed in some patients.
• Thromboembolism (in about 40% of cases) observed in patients is explained by the formation of a molecule similar to coagulation factor X by tumor cells.
The so-called 4D syndrome is characterized, which consists of diabetes, dermatitis, deep venous thrombosis and depression.
How to recognize diabetic neuropathy
Pathogeny of necrolytic migrans erythema in pancreatic tumor
One theory is that erythema migrans necrolytic (NME) may be caused by a decrease in tryptophan in the skin due to excess circulating glucagon. Tryptophan is responsible for the functioning of nicotinic acid, which regulates the cellular composition, capillary tone, the formation of the epidermis and mucosal epithelium.
According to another theory, NME is associated with hypoalbuminemia due to excess glucagon. Albumin is a transport protein for zinc and essential fatty acids. Zinc plays a fundamental role in maintaining skin trophism and prostaglandin synthesis.
Interesting endocrinology: hormonal aging of the body
Necrolytic erythema migrans as a visual sign of pancreatic tumor
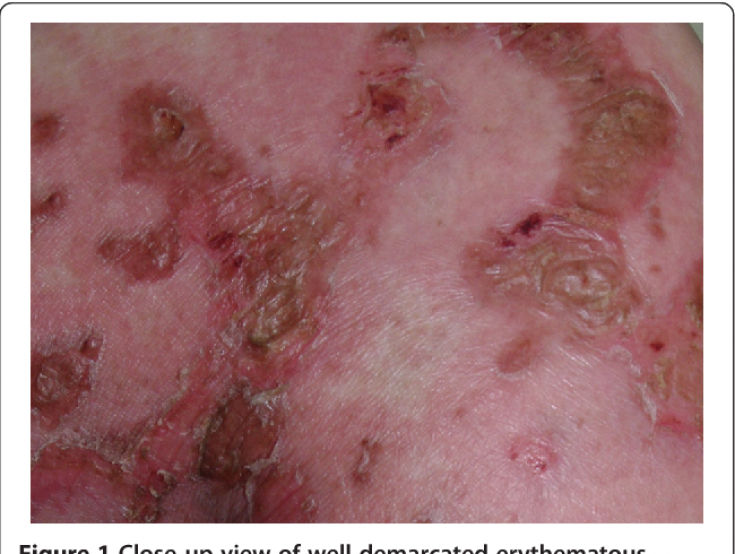
The skin manifestations of erythema necrolitica migratory include maculopapular, annular lesions and blisters whose lid collapses after a few days. Pustular transformation due to bacterial superinfection is possible. Lesions often coalesce, heal with hyperpigmentation.
NME initially appears in areas of the skin that are subject to friction and trauma, such as the legs, arms and forearms, as well as the buttocks, pubic area, groin area and perineal area. Atrophic glossitis, commissural cheilitis, stomatitis, balanoposthitis or vulvovaginitis often develop.
The hormone melatonin may increase the risk of diabetes

Diagnosis of a pancreatic tumor producing glucagon
1. Determination of the level of glucagonemia by radioimmunoassay (RIA) is mandatory. A positive test result for glucagonoma is greater than 1000 pg/mL (reference range is 50-200 pg/mL).
2. It is important to test your fasting blood sugar.
3. A complete blood count is important in assessing the presence of anemia.
4. Because glucagonoma can rarely be part of multiple endocrine neoplasia type 1 syndrome, serum insulin, glucagon, prolactin, calcium, and vasoactive intestinal polypeptide (VIP) levels are also checked.
The prevalence of glucagonoma is 1.3% of pancreatic cancer, but doctors assume a higher actual incidence.
5. Serum concentrations of amino acids, zinc and essential fatty acids should be examined to confirm nutritional deficiencies.
6. Determination of the level of transaminases, bilirubinemia and alkaline phosphatase is important for the detection of liver metastases.
7. Detection of telomerase and quantification of the human telomerase reverse transcriptase (hTERT) protein subunit has been proposed to distinguish between clinically benign malignant endocrine tumors.
8. In clinical practice, hTERT protein ribonucleic acid (mRNA) quantification has been used to quantify malignancy.
9. Ultrasound, angiography, computed tomography (CT) and magnetic resonance imaging (MRI), Metaiodobenzylguanidine scintigraphy, pancreatic tumor biopsy.
Diabetic Foot: Treatment of Ulcers with Nitric Oxide Dressings
Treatment of pancreatic tumor producing glucagon
• If possible, surgical resection procedures are performed.
• Condition control is possible in the early stages of the disease with somatostatin analogs (octreotide, lanreotide).
• Peptide receptor radionuclide therapy (PRRT) with 177Lu DOTATATE has been proposed as first-line therapy in patients with glucagonoma and metastases.
• Glucagonoma patients who have severe weight loss may require a period of total parenteral nutrition as part of preoperative preparation.
• Antibiotics, steroids, amino acids and zinc ointments are applied topically to the affected skin.
• Venous thrombosis prophylaxis and low-dose subcutaneous heparin are mandatory for all patients during the preoperative period.
• Patients for whom surgery is not an option are given streptozotocin and doxorubicin or streptozotocin and 5-fluorouracil.
• In patients with widespread metastases, hepatic artery catheterization is performed to infuse doxorubicin, cisplatin, and mitomycin-C.
How does the skin react to a lack of thyroid hormones
Prognosis of a patient with a pancreatic tumor
Glucagonoma has a slow growth rate. Most cases begin with non-specific symptoms, with an average delay in diagnosis of 3 years. Approximately 50% of cases are complicated by liver or regional lymph node metastases at diagnosis.
Nevertheless, targeted detection of pathology and a modern arsenal of diagnostic measures allow timely diagnosis of a pancreatic tumor. Large-scale studies are being conducted to determine the effectiveness of various approaches to the treatment of glucagonoma.
You may be interested in an article on our website estet-portal.com in the section "Endocrinology" Morning hypoglycemia. How not to miss insulinoma?
Adapted from Medscape
You may be interested in: Diagnosis and treatment of benign breast tumors.
Share:





Add a comment