
Rehabilitation of patients who have undergone surgery on the maxillary sinuses and require repeated operations causes some difficulties in terms of pre-implantation preparation (sinus lift, augmentation). This is due to the high probability of a negative result of such operations due to the presence of inflammatory, post-traumatic and cicatricial changes both in the mucous membrane and in the bone walls of the maxillary sinus. With the introduction of endoscopy techniques, sinus lift surgery has become less dangerous and more effective.
Advantages of endoscopic methods in sinus lift surgery
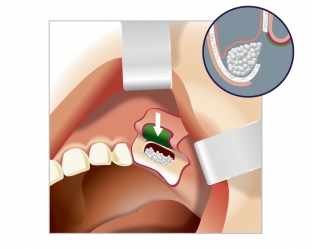
With a long absence of teeth on the lateral surfaces of the upper jaw, its bone tissue atrophies. To install an implant in the upper jaw, a certain thickness of bone tissue is needed for reliable implant attachment. If it is insufficient, an increase in the bone tissue of the upper jaw is carried out, which is called sinus lifting. Sinus lift surgery refers to bone grafting and is a procedure that, in some cases, is performed before dental implants. During a sinus lift, the doctor lifts the bottom of the maxillary sinus shell and inserts bone or osteoplastic material into the resulting space.
One of the methods that allows you to additionally control the course of the operation on poorly visible areas of the sinus during sinus lift surgery is the endoscopy method. Such control is possible not only through the created window in the anterior - lateral wall of the sinus, in the zone of detachment of the mucous membrane from the bone walls, but also from the side of the nasal cavity (through the natural anastomosis, rhinostomy).
Endoscopic methods of diagnosis and treatment are increasingly used in surgery. The first publications on the use of endoscopic techniques in maxillofacial surgery appeared at the end of the last century.
The endoscopic method has shown a high level of effectiveness in sinus lifting, as well as in the treatment of:
- inflammation of the maxillary sinus;
- temporomandibular joint;
- during osteosynthesis of mandibular fractures;
- when facelifted;
- when removing cysts and foreign bodies from the maxillary sinuses and in the treatment of odontogenic maxillary sinusitis.
Identification of risk groups during sinus lifting
Access to the maxillary sinus through a natural anastomosis is essential in the case of sinus debridement in the presence of signs of chronic sinusitis, cysts or foreign bodies. This allows sinus lift to be performed simultaneously or to be performed earlier than with access to the sinus through the anterior wall, when the mucosa has to be perforated to penetrate it. In this case, a sinus lift can only be performed 6-8 months after the previous operation.
Patients with chronic maxillary sinusitis, maxillary fractures, or a history of sinus surgery who are scheduled for dental implantation, sinus lift, or augmentation should be considered at risk.
Research on the efficacy of endoscopy in sinus lift surgery
Six sinus lift operations were performed under endoscopic control through the middle nasal passage in patients at risk. The mean age of the patients was 38.5 years. About 3 years ago, 2 patients underwent maxillary sinusectomy, reposition and fixation of fragments after a Le Fort II fracture of the upper jaw. 4 patients had diagnosed maxillary sinusitis. In 2 patients, cysts were first removed through the maxillary junction, and in one patient, a foreign body (filling mass) was removed from the maxillary sinus, and then a sinus lift was performed. Operations were performed under local anesthesia.
Sinus lift procedure using endoscopy
In the work, an endoscopic complex was used, which consisted of endoscopes, a set of instruments for endonasal surgery, a shaver system and a portable drill. During the sinus lift, endoscopic technique was used to control the detachment of the mucous membrane from the bone walls from the side of the natural anastomosis through the bone window in the anterior - lateral wall.
At the same time, perforations of the sinus mucosa were detected in 2 patients. During the closure of the perforation sites with the BioGide membrane and the filling of the formed cavity with Bio Oss granules, the correct installation of the membrane and the sufficiency of filling the cavity with granules were monitored using an endoscope. The excess material that got into the sinus cavity was immediately sent through the natural fistula. The postoperative period proceeded without complications. Surgical wounds healed by primary intention.
Thus, the use of endoscopic technique during sinus lift operations in patients with chronic sinusitis and consolidated fractures of the upper jaw is relevant and justified. This allows you to control the course of the operation from the side of the sinus and directly in the area of surgical intervention at all its stages.
Share:






Add a comment