

Pperiorbital zone ("area around the eyes") is a complex of soft tissues surrounding the orbit, which are associated with its bony boundaries (points of fixation of muscles and connective tissue skeleton), as well as neurovascular bundles that provide blood supply and innervation of soft tissues.
Read on estet-portal.com what Dr. Zoya Divan has to say (Zoya Diwan) about the vascular anatomy of the eye and periorbital area, knowledge of which is necessary to prevent vision loss after the introduction of fillers.
- Major arteries supplying blood to the eyes and periorbital area
- What are the specifics of vascular anatomy that should be taken into account when working with fillers
- Vision loss after fillers: causes of complications
- Emergency methods in case of complications after fillero injectionin
Major arteries that supply blood to the eyes and periorbital region
The main artery that provides blood supply to the eye is the orbital (GA). The location of the multiple branches of GA varies from patient to patient.
For example, in 3% of people, the GA originates from the middle meningeal artery, a branch of the external rather than the internal carotid artery.
GA supplies blood to two separate zones – orbital (mainly eye socket) and periorbital (mainly muscles and around the eyes) – see Table 1.
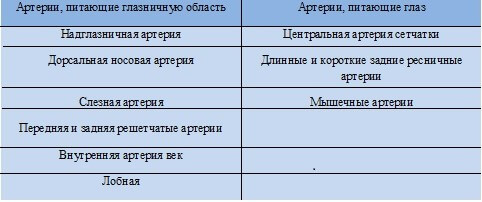
Table 1: Branches of the ophthalmic artery supplying the eye and orbital region
The internal carotid artery, as a rule, passes through the cavernous sinus and forms a branch – orbital artery, which enters the orbit through the optic opening.
The external carotid artery has two branches that supply the orbit with blood: the infraorbital and middle meningeal arteriesand.
What features of vascular anatomy should be considered when working with fillers
Several arterial lesions associated with dermal fillers are associated with an increased risk of developing complications.
Occlusion of the long and short posterior and anterior ciliary arteries can result in symptoms of anterior ischemic optic neuropathy, including vision loss due to reduced or cessation of ciliary blood supply, in particular the head of the optic nerve, which is fed by these arteries.
Filler Complications: A Guide for Specialists by Dr. Patrick Tracy
Supraorbital and dorsal nasal arteries – terminal branches of the ophthalmic artery; the introduction of a filler into these arteries can lead to the formation of an embolus, which, with the reverse flow of blood, can move to any of the arteries that directly supply blood to the optic nerve or retina of the eye.
It is important to understand that there is a huge network of anastomoses between these arteries.
Diagram 1 shows the location of the major arteries that supply blood to the eyes and orbit. All of these arteries are branches of the ophthalmic artery. All branches of the ophthalmic artery and its anastomoses with other branches, as well as with the arterial branches of the external carotid artery (ECA) are shown. These include branches of the ECA that anastomose with branches of the internal carotid artery (ICA).
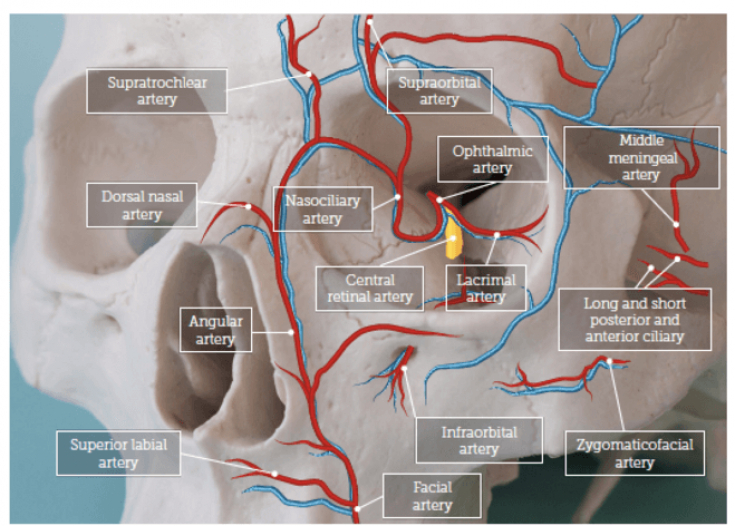
Diagram 1: Major arteries surrounding and supplying the orbit
|
|
Follow us on
Instagram! Another example is the injection of the drug into the angular artery during the introduction of a filler into the nasolabial fold. This can lead to
filler embolizationof the dorsal nasal artery, which anastomoses with the angular artery and ultimately opens up access to the HA. The most dangerous area in the context of filler correction is between the eyebrows – almost 40% of the 98 recorded cases of visual loss occurred after the introduction of drugs in the interbrow area.
Under the pressure of the syringe, the filler passes through the HA, and after the pressure stops, the systolic pressure in the HA pushes the embolus into the branch of the HA, including the central retinal artery, which can lead tovision loss
. Thus, the risk of loss of vision exists when
dermal fillersare injected into almost any area of the facea. Loss of vision after fillers: causes of complications and actions in case of a complication
Loss of vision usually occurs within seconds of the affected artery being affected.
If the
central retinal arteryis affected, the loss of vision becomes irreversible after an hour and a half (according to the results of a study conducted by C.J . Hwang et al. in 2019). However,
S. Tobalem et al. in 2018 conducted a literature review and found that the response time is much less – only 12–15 minutes.
pain;
sudden loss or blurred vision;- ptosis and weakness/paralysis of the eye muscles (ophthalmoplegia).
- The above symptoms occur due to
- impaired blood flow to the multiple arteries surrounding the eye, including the supra- and infraorbital.
Cosmetologists Guidelines: The Dublin Complications Protocol
According to the results of meta-analysis conducted in 2015 by
Dr.K. Beleznay 98 cases of loss of vision after injections of fillers (including autologous fat, hyaluronic acid, poly-L-lactic acid and calcium hydroxyapatite. In 38 out of 98 cases, vision loss occurred after the introduction of fillers in the zone between the eyebrows; also the most dangerous in the context of this complication are
areas of the nose, nasolabial fold and forehead.There is a risk of loss of vision when dermal fillers are injected into almost any area of the face. For
preparations, almost 50% of patients were injected with autologous fat, 23.5% with hyaluronic acid, the remaining cases were with poly-L-lactic acid, paraffin, polymethyl methacrylate, silicone oil and calcium hydroxyapatite.
In 11 out of 98 cases, the complication arose during the correction of the periorbital zone (including the nasolacrimal trough and cheeks).
In most cases, vision, unfortunately, could not be restored. Complications from the nervous system were recorded in 23.5% of cases. A similar study was conducted by the authors in 2019, which identified 48 new cases of
partial or total loss of visionafter filler injections between January 2015 and September 2018
In 81.3% of cases, complications occurred after the introduction of HA-based fillers. In 10 cases, a complete restoration of vision was reported, in eight – o partiallym.
Methods of emergency care in case of complications after the introduction of fillers Timely interventions, including
hyaluronidase injectionsand
massage of the affected area, have been shown to be effective in restoring or partially recirculating the eye area in some patients. Prevention and treatment of complications of aesthetic correction in the periocular region
andKing have compiled a list of actions to be taken by the practitioner if this complication occurs: If the patient complains of pain in the eye or sudden loss of vision, the procedure should be stopped immediately
.- Move patient to supine position.
- Contact ophthalmologist.
- Before the arrival of the ophthalmologist, reduce intraocular pressure with 1–2 drops of 0.5% timolol, give the patient to breathe into a paper bag and 300 mg of aspirin
- . Try to eliminate the embolus by massaging the eye.
- Inject a dose of hyaluronidase into the treated area (retrobulbar injections are performed by an ophthalmologist only for 90 minutes).
- In addition to the above, the Aesthetics Interventional Induced Visual Loss (AIIVL) Consensus Group recommends the sublingual application of glyceryl nitrate in spray form.
Adapted from Aesthetics.
Share:





Add a comment