

Contour plastic surgery of the upper third of the face is associated with a number of risks – both controllable (eg, hemorrhage) and, in some cases, irreversible (blindness). Therefore, knowledge in the field of facial anatomy for cosmetologists performing correction with neuromodulators and dermal fillers tops the list of the most important conditions for the safety of injection procedures. In this article estet-portal.com Tracey Hotta talks about important aspects of the anatomy of the upper third of the face: the location and function of muscles, blood vessels and nerves in the forehead, between the eyebrows and temples.
- Anatomy of the forehead area: frontalis muscle, blood supply, innervation
- Anatomy of the glabellar area: glabellar complex, major arteries
- Anatomy of the temporal zone: temporalis muscle, vessels, fasciae
Anatomy of the forehead area: frontalis muscle, blood supply, innervation
Frontal muscle (m. frontalis) – a large muscle that is located on the forehead and raises mainly the central part of the eyebrow.
The frontalis muscle originates at the hairline, from the cranial aponeurosis. The point of attachment is located at the level of the eyebrows, where its fibers are intertwined with muscle fibers:
- proud;
- eyebrow wrinkler,
- lowering an eyebrow;
- circular muscle of the eye.
Contraction of vertical muscle fibers m. frontalis over time leads to the appearance of horizontal wrinkles in the forehead area. At the temporal line, the frontalis muscle is partially located above the temporal.
Subscribe to our channel in Telegram!
Correction of the functional frontalis muscle can lead to "heaviness" of the or ptosis of the eyebrow. Relaxation of the frontalis muscle without its direct correction can be obtained by correcting the depressor action of the glabellar complex, the fibers of which are intertwined with m. frontalis.
provided by:
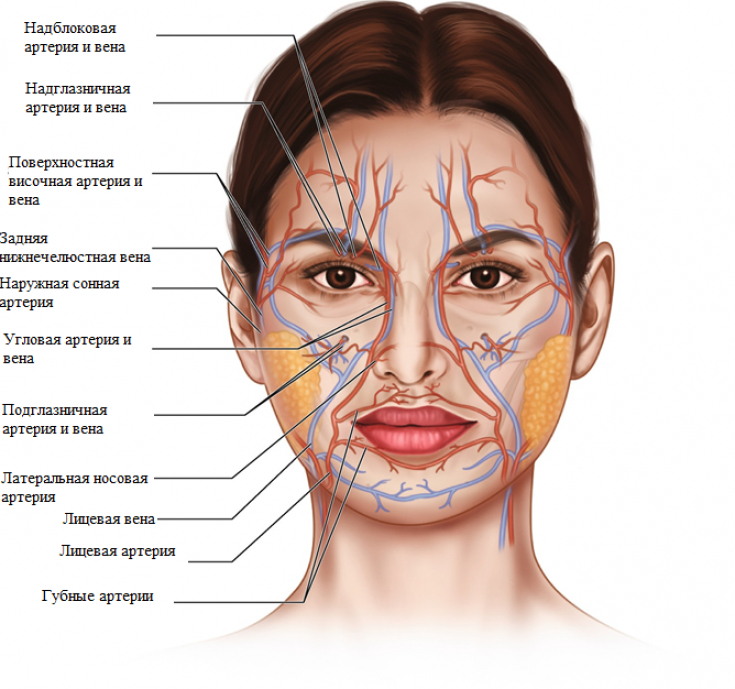
frontal branch of the superficial temporal artery (lateral);- supratrochlear artery (medally);
- supraorbital artery (medially).
emerges from the external carotid in the area of the lower jaw, ascends about 1 cm opposite the ear in the preauricular space and crosses the zygomatic arch (anterior branch of the superficial temporal artery).
Because m. frontalis – the only levator muscle of the upper third of the face, it is important to evaluate its function before botulinum toxin injections.frontal branch
– the terminal branch of the superficial temporal artery, which anastomoses with the supraorbital arteries in the region of the frontalis muscle. The supratrochlear and supraorbital arteries emerge from an opening located in the orbital ridge. 2.7 cm. These blood vessels exit through the muscles that lower the eyebrows and ascend to enter the frontalis muscle about 2 cm above the orbital ridge. Read also:
Forehead anatomy for injectionists: important nuances of the structure and correction of the zone responsible for the innervation of the frontalis muscle is the temporal branch of the facial nerve. The nerve emerges from under the parotid gland and passes upward through the zygomatic arch. It is located in loose connective tissue under the temporoparietal fascia. The nerve emerges from the deep plane into the superficial one as it crosses the lower surface of the frontalis muscle at the temporal line. The frontal cord of the superficial temporal artery
passes above the nerve. Anatomy of the glabellar area: glabellar complex, major arteries
The glabellar complex of muscles in the area between the eyebrows consists of:muscles of the proud (procerus
);- eyebrow wrinkling muscle (corrugator supercilii);
- muscle that lowers the eyebrow (depressor supercilii).
- The brow pucker originates at the medial brow ridge on the frontal bone and enters the skin of the medial brow. The supratrochlear neurovascular bundle exits through corrugator supercilii and provides sensitivity and blood supply to the central part of the forehead. The puckering brow muscle compresses the medial part of the brow.
In 2012, Pessa and
Rohrichfound that fat tissue compartments in the glabellar complex result in vertical lines (folds). The beautician can use these folds as indicators of the position of the supratrochlear artery and nerve. When the brow complex is reduced, three folds: median;
corrugatory;- supraorbital.
- There are fat compartments between them – medial and lateral. The location of the supratrochlear artery is indicated by the corrugator, and the supraorbital – supraorbital fold respectively.
Facial anatomy for injectionists: how not to damage facial nerves when injecting dermal fillers The supratrochlear artery runs under the brow-pucker muscle and the frontalis muscle, its superficial marker being the corrugator fold. As it travels upward through the frontalis muscle, the supratrochlear artery emerges to the surface and passes just under the skin. This creates a risk of damage to the central vessel of the forehead and impaired collateral circulation during the correction of the area between the eyebrows.

Filler entering the supratrochlear artery can lead to
occlusion of the central retinal artery
and blindness. Therefore, injections are recommended in the area between the eyebrows:
superficial, directly under the dermis layer;
low concentration hyaluronic acid;- with low insertion force.
- This will help reduce the risk of bleeding and vascular damage.
Anatomy of the temporal zone: temporal muscle, vessels, fasciae
Temporalis(
m. temportalis) has a fan-shaped shape and is located laterally in relation to the orbital ridge and above the zygomatic arch. M. temporalis intertwines with the chewing muscle and participates in chewing process. The temporal cavity appears as a result of:
reabsorption of bone tissue;
muscular atrophy;- deflation of the fat package in the temporal zone.
- This results in drooping of the lateral brow and skeletalization of the face.
- The temporal zone consists of
: deep and superficial. The deep temporal fascia is separated from the superficial avascular plane by loose connective tissue. It attaches securely to the periosteum near the border of the temporalis muscle, but not to the zygomatic arch. The fascial layer closely adheres to the muscle and is not very pliable, especially in younger people. This factor must be taken into account when
correction of the temporal zone with fillers. With age, the muscle under the temporal fascia atrophies, increasing the space for filler augmentation. In the area of the temporal cavity, you can use two techniques of gel injection:
Deep insertion into the periosteum with a needle;
Introduction of cannulas into loose connective tissue between two layers of fascia.- When working with the first technique, the location of the deep temporal arteries must be taken into account. Blood enters the temporal zone through two branches of the maxillary artery –
- anterior and posterior deep temporal arteries , as well as a branch of the external carotid artery –
. In the temporal fossa, the posterior deep temporal artery and the deep temporal nerve enter the temporalis muscle. The artery supplies blood to the upper part of the temporal bone, the periosteum of the skull, and also to the temporalis muscle.

.
The temporal filler is injected into muscle, not bone. The temporal muscle is closely connected with the periosteum. Since the deep temporal arteries run in the muscle, it is recommended to perform an aspiration test before injections.
Temporal area augmentation may result in temporary visualization of vessels until the product is integrated into the tissue.
Second techniqueused fortemporal cavity augmentation
. The filler is injected with a needle or cannula into the loose connective tissue located between the two layers of the fascia. The frontal branch of the superficial temporal artery and vein, as well as the temporal branch of the facial nerve, are located in the superficial temporal fascia. When inserted correctly, movement of the needle or cannula under the vessels is observed. Knowledge of the anatomy of the upper third of the face – location of muscles, nerves and blood vessels of the frontal, brow and temporal zones – will help the beautician to carry out injection procedures as safely as possible and obtain the optimal correction result. Adapted from Plastic Surgical Nursing.
More interesting videos on ourYouTube
-channel!
Share:




Add a comment