
The issue of choosing the most effective filler that can smooth out wrinkles, improve skin quality and provide the maximum rejuvenating effect, is constantly discussed by aesthetic medicine specialists. New techniques are being developed, both the effect of fillers and the survival rate of subcutaneously injected autologous fat are being studied.
 We offer readers of estet-portal.com one of the articles by Belgian plastic surgeon Alex Verpaele, director of the Coupure Center for Plastic Surgery (Ghent), in which he describes the SNIF facial rejuvenation technology.
We offer readers of estet-portal.com one of the articles by Belgian plastic surgeon Alex Verpaele, director of the Coupure Center for Plastic Surgery (Ghent), in which he describes the SNIF facial rejuvenation technology.
The action of fillers depending on their origin
Skin aging is a process that depends on many factors. In addition to external and internal causes of aging, repetitive facial movements are an important mechanical factor contributing to the formation of wrinkles. As with a hinge that bends in the same place, the muscular movements that shape the facial expression create lines on the surface of the skin. At first, these lines can only be seen during contraction (dynamic wrinkles). But the regular repetition of these movements over time makes these lines permanently visible (static wrinkles).
Wrinkles can be eliminated by filling the subcutaneous and intradermal planes. Filling in the subcutaneous plane is used to eliminate deep wrinkles and folds resulting from thinning of the subcutaneous volume. In contrast, small wrinkles are treated with intradermal injections, as they are the result of changes in the skin itself.
Since early experiences with filling materials, clinicians have searched for the perfect filler. An ideal skin filler should not have teratogenic, oncogenic properties, but should be as compatible as possible, while having a minimum of side effects. Availability and cost are important criteria. It is also necessary to take into account the durability of the result of the filler. The filling materials may be autologous or heterologous in origin. Autologous materials are taken from the patient's own body (such as fat and skin grafts). Heterologous fillers do not originate from the patient's body, but can replace human body substances such as collagen and hyaluronic acid. Collagen heterologous fillers can also be xenogenic (of animal origin) or allogeneic (of human origin).
Side effects of fillers and how to solve these problemsIn previous studies with heterologous dermal fillers, biocompatibility and allergic reactions have been heavily emphasized, but modern fillers are less allergenic or even non-allergic.
Bruising, redness and swelling may occur around the injection site, but these problems disappear after a few days. From time to time, after a few months, side effects may appear in the form of subcutaneous granulomas, which sometimes remain for a long time. These problems most commonly occur with permanent fillers and are more difficult to resolve. Other problems that may occur are chronic edema, lymphadenopathy, scarring, and even skin ulceration.
Peculiarities of choosing filler – fillers and autologous fat
As noted earlier, filler availability and cost are important issues. The obvious advantage of pharmaceutical excipients is the ability to use them in finished form, but such products are usually more expensive. In contrast, deep facial fat grafting has been used for years in facial rejuvenation and at a lower cost.
Fat grafting by injection was first performed in 1910 by Hjolender to correct atrophy. Modern fat injection techniques were popularized and described by Coleman. They are characterized by partial absorption of the injected fat during the first 6 months, a relatively small number of complications and unsuccessful results, as well as a slight soreness of the procedure in the donor area. The amount of fat required for intradermal injection is very small (0.5-5 ml). If intradermal fat grafting is performed without deep lipofilling, fat collection does not take much time (2.5-25 ml), and the choice of the donor area rarely creates problems even in very thin patients.
Specificity of SNIF technique of fat insertion with a needle
Based on the research of previous authors, combined with modifications and refinements of previously described techniques, we have developed the SNIF technique, the aim of which is to collect as small fat particles as possible. We use 2-3mm diameter fat collecting cannulas, which contain a large number of small diameter (1mm) sharp holes. The fat is then filtered through a sterile nylon cloth with a mesh size of 0.5 mm. We started using this technique even before the "closed" systems became available and showed good results at a low cost of the procedure, so we continue to use it.
The filtered fat can then be easily injected through a 23 gauge needle. The 23G size was necessary because the prepared fat cannot be injected through smaller diameter needles without constant interruption. The key to successful fat grafting is the use of micrografts. The radius of a fat particle is inversely proportional to its contact surface. This means that for the same volume of injected fat, halving the diameter will double the contact surface (Fig. 9).
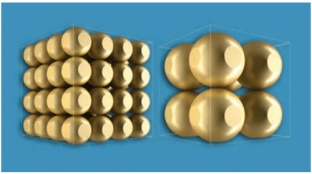
Fig. 9. For a given volume, the radius of the fat particles is inversely proportional to the contact surface. By reducing the size of the particles, we increase the size of the contact surface with the surrounding capillaries
The larger contact surface of the fat means better contact with the capillaries at the injection site and therefore a higher level of graft viability, which reduces the likelihood of the need for re-correction.The main problem with the sudden injection of soft tissue fillers are cases of intravascular injections followed by embolization of certain vascular areas. This can lead to necrosis of the skin at the injection site, or even more catastrophic consequences such as blindness or stroke.
When working on the face, we always prepare the surgical surface with an injection of a local anesthetic solution containing adrenaline, whether the patient needs local or general anesthesia (lidocaine 0.3%, adrenaline 1/650,000). This is important because epinephrine-induced vasoconstriction minimizes the risk of intravascular injections and reduces bruising to some extent. The injection is always carried out in the superficial plane of the skin during needle withdrawal, again to minimize the risk of intravascular penetration. In addition, compressing the skin (the fold should be pinched between the index finger and thumb) during the injection will help to occlude any vessel near the injection site. Classical (deep) subcutaneous fat grafting is always done with a blunt cannula.
Side effects of fillers and injected adipose tissue
In our patients who have undergone intradermal fat injections followed by laser resurfacing (Erbium: YAG), the result of superficial resurfacing has always been significant because wrinkle filling has already been achieved. When laser resurfacing is combined with intradermal fat injections, the effect is synergistic. This observation contradicts the claim that laser resurfacing of skin recently treated with a heterologous dermal filler can cause degradation or liquefaction of the filler material. Intradermal fat injections have also become a viable alternative for patients seeking skin rejuvenation without laser resurfacing.
Another advantage of fat injection is the use of autologous material that does not degrade over time, thus making the result more permanent. In addition, fat injections are not associated with the problems that are common with non-autologous permanent fillers. During the time that our SNIF procedure was applied, very few problems were found - and all minor (redness, swelling and bruising). Bruising was the most common adverse effect (38% of patients). No significant issues noted.
Possible problems that can be caused by classic (deep subcutaneous) fat grafting include palpable nodules, indurations, fat necrosis and fatty cysts. None of these complications have been reported in patients, possibly due to the fact that small amounts of small fat particles were injected and they were injected into well vascularized tissue.
The limited value of this study lies in the lack of quantitative analysis of the results. They were compared only with our own clinical experience with absorbable synthetic fillers. This technique is proposed as a valuable addition to the current list of skin filling procedures.
Detailed description of SNIF technique of fat injection with a needle will be presented at the ISAPS World Congress, which will be held in Kyiv on May 19-20,
ALEX VERPAELE, BELGIUM
- Developer of the revolutionary MACS lift
- Member of the International Association of Aesthetic Plastic Surgeons ISAPS
- Member of the American Association of Aesthetic Plastic Surgeons ASAPS
- Member of the Royal Belgian Society for Surgery
- Member of the Belgian and Dutch Association of Plastic Surgeons
- Founder of Aesthetic Medical Center 2 «(E: MC²), Sint Maartens-Latem
- Director of the Coupure Center for Plastic Surgery, Ghent
the technique of the SNIF procedure and see some of the results achieved in patients using the surgical technique of Alex Verpaele .
Share:






Add a comment