

Urinary incontinence is not only a psychologically extremely painful issue for women, but also a very common problem that occurs to one degree or another in every second patient over the age of 40. However, age-related changes in the structure of the pelvic floor are far from the only factor in the development of this disease.
The primary place in its formation is occupied by birth trauma, especially in the case of repeated births or the birth of large children. With age, the risk of urinary incontinence increases steadily and, according to some estimates, can reach 75-80% in patients older than 50 years.
 Tatiana Vitalievna Shevchuk, Head of the Department of Gynecology, Medical Club Clinic
Tatiana Vitalievna Shevchuk, Head of the Department of Gynecology, Medical Club Clinic
Why urinary incontinence occurs and how to deal with it
Stress urinary incontinence – it is its involuntary loss during physical exertion, coughing, laughing, sneezing, jumping, sexual intercourse, etc., that is, in situations accompanied by an increase in intra-abdominal pressure. In the presence of impaired fixation of the urethra, the influence of these factors leads to loss of urine on exertion.
Today, the "gold standard" in the treatment of stress incontinence (stress incontinence) is staging free synthetic loop (TVT-O, tension-free vaginal tape). This mini-surgery has been performed on more than 200,000 women in the last 5 years.
Its significant advantages are low trauma, high efficiency, life-long effect, speed of execution and the possibility of performing under various types of anesthesia, which makes it popular and possible even for older women. The effectiveness of this operation in the treatment of stress urinary incontinence is 90-97%.
The duration of such an intervention is 15-20 minutes, and it can be performed both under anesthesia and under spinal anesthesia, and in case of concomitant prolapse of the pelvic organs, it can be supplemented with a vaginal plasty. Length of stay in hospital – usually up to a day. Return to full activity (including sexual activity, water procedures and physical activity) occurs within 2-3 weeks after the operation.
Read related : "Stress Urinary Incontinence"
The essence of the surgical operation performed for urinary incontinence
The operation consists in passing and placing under the urethra a braided tape (loop, sling) made of synthetic material Prolene, which provides support and fixation of the urethra and eliminates its excess mobility. For its introduction, 3 minimal skin punctures (about 1 cm long each) are made - under the urethra and on the inner surfaces of the thighs (in the region of the inguinal folds), which are sutured with absorbable suture material and leave virtually no traces (Fig. 1, 2).
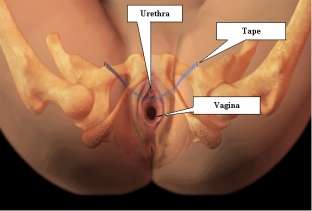
Fig. 1 Location of the loop in the tissues of the pelvis (anterior projection)
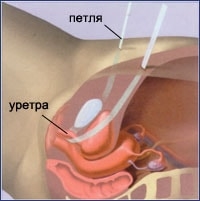
Fig. 2 The location of the loop in the tissues of the pelvis (lateral projection)
Prolene is a unique modern material that is not amenable to resorption processes, does not cause inflammatory and allergic reactions. The weaving of this tape is thought out in such a way that the size of its pores allows the passage of connective tissue cells of fibroblasts that produce fibrin - connective tissue scaffold protein.
Over time, this implant "sprouts" connective tissue fibers and becomes a matrix that strengthens the urethra and keeps urine in the bladder even with strong pressure in it (for example, when coughing, laughing, sneezing, etc.). That is why the full therapeutic effect of the loop may not fully occur immediately, but within 1-6 months after its setting.
Possible complications after urinary incontinence surgery
As with other types of surgery, complications are possible with this implant. Here are the most common of them (given on the basis of world statistics).
- Functional impairment
- Postoperative pain can occur in the perineal, groin, lower abdomen, at the level of the hip joints, legs, feet - 15-20%.
- Disorders during urination (prolongation of the act of urination, impaired sensitivity, curvature of the urine stream, the need for additional straining, incomplete emptying of the bladder) - & nbsp; 5-15%.
- Formation of an overactive bladder (frequent, pronounced urge to urinate) - 5-10%.
- Structural disturbances
- Insufficient efficiency of the operation – 10-15%.
- Formation of erosion (exit) of part of the loop into the vagina or urethra – 1-5%.
- In the case of a patient with mixed urinary incontinence (stress and urge), this operation does not lead to a decrease in the symptoms caused by urge incontinence (frequent irresistible urge to urinate during the day and at night). Medications are used to treat this type of incontinence.
- Inflammatory diseases of the genitourinary tract - 1-5%.
- Infection of the implant, which may lead to the need for surgical treatment or its removal - 1%.
Most functional complications, as a rule, resolve on their own within a period of several days to 6 months and do not always require additional therapy.
For women of reproductive age, it should be noted that if they plan to become pregnant after surgery, given the impossibility of stretching the TVT-O during vaginal delivery, they are recommended delivery by planned caesarean section.
Share:





Add a comment