
The arsenal of practicing surgeons is constantly replenished with various tools for the correction of functional and cosmetic problems in the middle part of the face. Among them: lifts of various degrees of aggressiveness, blepharoplasty to correct the position of the lower eyelid and preserve its youthful shape, removal and reposition of fat in the lower eyelid area, various implants for the zygomatic and orbital zones, replenishment of volumes using autologous adipose tissue and fillers available on the market. At the same time, the surface of the skin remains a separate task – wrinkles and sagging skin require action on the surface of the skin to compress collagen and tighten the skin. For this, laser and radio frequency devices are successfully used. In this article, Dr. Fred Fedok – plastic surgeon from USA –
Correction of the middle third of the face: the anatomy of age-related changesConsidering the mechanisms of aging
of the middle part of the face, which must be taken into account when choosing procedures for correction, the doctor draws attention to three main anatomical zones:
- lower eyelids;
- connection of lower eyelids and cheeks;
- directly cheeks.
Various dynamic factors that affect midface aging include:
- reduction of skin elasticity;
- stretching of the retaining ligaments in the cheeks and orbit, which are connected to the skeleton, muscles and skin itself;
- involutional changes in fat compartments, which are the result of weakening of their supporting structures and directly atrophy of adipose tissue.
As a result of the above changes there is a drooping of the edge of the eyelid, the orbicular muscle of the eye lengthens vertically, as a result of which wrinkles appear under the eyes, and the cheek fat is shifted downward (Fig. 1).
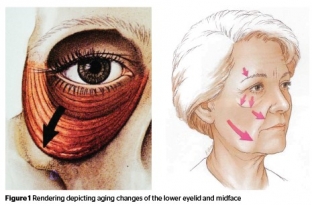
Fig. 1. Age-related changes in the lower eyelid and middle third of the face
The nasolabial fold becomes more pronounced, but not due to its deepening, but due to the displacement of the zygomatic tubercle down, closer to the nasolabial fold. Thus, due to the contrast, the fold visually looks more pronounced.A characteristic deformity appears at the junction of the lower eyelid and cheeks – double bulge of the lower eyelid and midface junction (Fig. 2). Such deformation is a consequence of changes in the volume of bone and soft tissues in the periorbital and zygomatic regions, as well as soft tissue ptosis.
On a young face, this anatomical region has even contours and is presented as a gradual transition from the contour of the lower eyelid through the orbital ridge to the cheek. With age, these structures separate from each other, and their contours become more visible.
The above changes are more pronounced in patients with insufficient bone projection of the orbital ridge and midface, resulting in the formation of a negative vector (Fig. 2). Signs of midface aging appear earlier in these patients. Insufficient support of periorbital structures results in:
- unaesthetic appearance of the lower eyelids;
- Skeletization of the orbital ridge;
- functional eyelid retraction;
- ectropion.
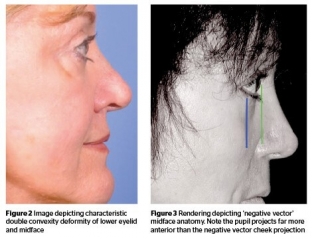
Fig. 2. (Left) Characteristic double bulge – deformity at the junction of the lower eyelid and cheek. (Right) "Negative vector" facial anatomy. The projection of the pupil is greater than the projection of the cheek.
And vice versa – in patients with good bone projection in the midface (or a positive vector), the periorbital structures are less prone to downward displacement due to age-related stretching of the retaining muscles of the cheeks.Modern methods of correction of signs of aging in the middle third of the face
The understanding of age-related anatomical changes, the popularization of new techniques and the development of new biomaterials have led to a change in the approach to midface correction. As a result, doctors manage to get better facial rejuvenation results compared to traditional facelift techniques. Due to the significant influence of this anatomical region on the appearance of the entire face, plastic surgeons pay special attention to the rejuvenation of its middle third. Modern cosmetic surgeons have a wide range of instruments to address a wide range of anatomical problems associated with aging. These include:
- volume restoration with fillers or autologous fat;
- blepharoplasty;
- lifting;
- correction of bone tissue.
The problem of soft tissue volume reduction and skeletonization, which lead, for example, to tear trough deformity, is in most cases solved with fat and fillers.
It is volume restoration that is the most common method of correcting the middle third of the face, especially in younger patients. Both injections of own fat and fillers available on the market give excellent results. But
fillers are more commonly used because they are non-surgical and less expensive.
Based on the patient's anatomical changes, an appropriate procedure can be selected for midface correction. In case of slight changes, it will be enough just to replenish the volumes:
- In patients with slight excess skin and wrinkles (no eyelid displacement), slight protrusion of fat in the lower eyelid area, slight skeletalization and downward displacement of the zygomatic fat pad, the author injects the filler along the eye fold (Fig. 3).
- For patients who have more pronounced changes with a noticeable downward shift of the malar fat pad, a slightly different volume replenishment strategy is chosen. As in the previous case, the filler is injected along the orbital ridge, but the contour of the cheekbones itself is also changed. Here, volume replenishment is carried out to lift the buccal tubercle. Improving the zygomatic contour also allows you to reduce the severity of the nasolabial fold. Gently inserted filler will smooth out the skeletalization of the orbital ridge, as well as the deformation of the lacrimal trough.

Fig. 3. (Left) before and (right) after HA filler injection along the infraorbital rim to correct tear trough deformity and skeletonization of the orbital rim
Ha-based fillers, which spread very well and have a slight lifting effect, are ideal for injection into the orbital region: they provide volume without the need for bone support; self-leveling in the tissues, which reduces the risk of lumpiness in the injection area.In the midface and lateral cheeks, it is best to use a HA with greater lifting effect and less spreadability to replenish volume and provide structural support. Such materials are injected deep, above the level of the periosteum. With proper assessment of the anatomy and choice of insertion technique, this procedure is safe, painless and with minimal risk of complications.
Autologous fat can also be injected into the zygomatic region (Figure 4). Deep fat injection makes the procedure simple, painless and safe.
Introduction of fat into the tear trough should ideally only be performed by experienced professionals, otherwise fat lumps will be visible through the relatively thin skin of the eyelids and can only be removed surgically.The safety of volume replenishment for the correction of the middle third of the face depends on the chosen injection technique and the correct assessment of anatomical changes.
The author typically injects HA fillers and patient fat into the midface using a blunt cannula to reduce the risk of bruising as well as intravascular injection.
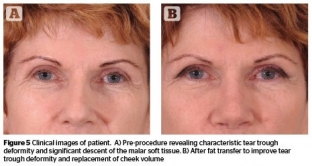
Fig. 4. Before (left) and after (right) fat grafting to correct tear trough deformity and fill cheek volume
Blepharoplasty for correction of the middle third of the faceExcess soft tissue and flabbiness in the treated area can be corrected through various surgical techniques:
- blepharoplasty;
- blepharoplasty with fat reduction;
- lifting (both transpalpebral and transtemporal).
Blepharoplasty should be performed in case of more pronounced signs of aging: excess skin on the eyelids, a large amount of protruding fat and shifting of the eyelid.There are many techniques for performing blepharoplasty. According to the author, it is best to choose transconjunctival or transcutaneous access for the operation. The choice of approach is based on the patient's anatomy and history of When a midface lift, eyelid retraction, ectropion correction or implant is required, the author prefers transcutaneous blepharoplasty in most cases.
Transcutaneous incisions are usually made below the eyelid, at least 4 mm from the lash line, to preserve the pretarsal region of the orbicularis oculi. The younger the patient, the closer the incision is made to the lash line. The medial part of the incision should be limited in order to preserve the innervation of the orbicular muscle of the eye.
Until the mid-1990s, the surgical approach to periorbital rejuvenation was limited to lower blepharoplasty, with soft tissue elevation of the eyelid, removal of excess skin and excess orbital fat. Later, blepharoplasty for the correction of the middle third of the face began to be performed with the reposition of the orbital fat (as a biological internal implant) on the orbital ridge.
In the case of a large amount of visually noticeable orbital fat, a certain part of it must be removed. With a significant tear trough deformity, the author removes the lateral fat pack and repositions the nasal and central fat packs over the ophthalmic fold.
Lifting options for correction of the middle third of the face
There are various techniques for performing mid-face lift procedures. Most often, surgeons use the transtemporal endoscopic approach to perform this procedure. Some lifting correction techniques are performed in conjunction with blepharoplasty through a transcutaneous or transconjunctival approach. The aim of a mid-face lift is to correct the contour and position of the lower eyelid, as well as to improve the junction of the eyelid with the cheek and to reposition the malar fat pad (Fig. 5).

Fig. 5. Before (left) and after (right) transtemporal/transpalpebral lift with correction of double convexity and elevation of the tubercle of the cheeks
Possibilities of bone tissue correction in rejuvenation of the middle third of the faceThere are also different implants made from biocompatible materials and intended for the correction of the middle part of the face and the orbital ridge. In patients with malposition of the lower eyelid and a negative vector, especially after a previous attempt at surgery, the author uses solid implants of the orbital ridge or zygoma.
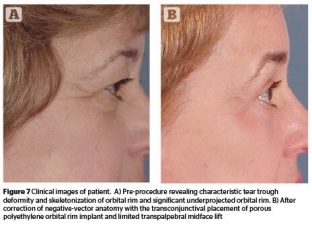
Fig. 6. Before (left) and after (right) correction of the "negative vector" by transconjunctival placement of a porous polyethylene orbital rim implant and limited transpalpebral lifting of the middle third of the face
Read also:The secrets of successful plastic surgery from Dr. Charles Randquist
The author has experience with porous polyethylene and silastic implants, which are placed using transconjunctival or transcutaneous access, in order to correct the negative vector of bone tissue (Fig. 6).According to Prime magazine.
Share:






Add a comment