
Purulent inflammation of the finger called pandactylitis covers not only the skin and subcutaneous tissue, but also spreads to the joints, tendons, and affects the bones. In a neglected state, pandactylitis can result in a mutilation operation for the patient. This disease is a complication of panaritium and develops most often due to errors of patients and doctors in providing assistance with panaritium. Pandactylitis may develop due to the late treatment of a patient with inflammation of the finger after a microtrauma or his indiscipline in following the course of panaritium treatment prescribed by the doctor.
The clinical picture of pandactylitis can be different depending on the location of the inflammation, the degree of neglect of the process and the nature of its prevalence. But in any case, the disease has the characteristic features – progressive melting and necrosis of tissues, loss of function of the inflamed finger.
Clinical case
Patient B, 40 years old
Anamnesis: works as a mechanic at an enterprise, during work he injured his thumb on the right hand in the area of the interphalangeal joint with a slipped tool. The patient treated the wound with iodine and sealed it with electrical tape, the next day at the first-aid post the wound was washed, the inflammation of the finger was treated with iodine and sealed with a plaster. Hot baths are recommended for the patient.
A week later, there is an acute pain, the finger is swollen, has lost mobility, purulent discharge has appeared from the wound. Patient released from work.
Diagnosis: articular panaritium of the first finger of the right hand.
Treatment: Penicillin injection at the base of the finger, antiseptic dressings, UHF.
No improvement. On the 16th day from the onset of the disease, soft tissues were dissected above the interphalangeal joint, there were purulent compartments. There is a phlegmonous process that extends to the joint and phalanges of the finger, tendon sheath. The patient is hospitalized.
Examination of the patient: temperature 38°, no pain, but the patient cannot hold his finger. There are fistulas with granulations, tissue necrosis, the skin is thinned and hyperemic, the tumor spreads to the wrist and palm. X-ray examination shows ostelmyelitis with sequestration, osteoporosis, lymphadenitis.
Diagnosis: pandactylitis.
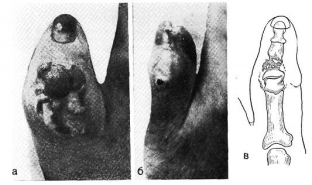
and —before the operation; b — after removing the bandage; in — x-ray diagram
Treatment: under anesthesia, granulations were excised and removed necrotic tissues, the nail plate was removed, the remnants of the extensor tendon and the articular capsule were excised. Abscesses are opened and fistulas are expanded.
After the operation, 2 weeks later, the edema disappeared, the wounds healed. The patient feels well. Sessions of ozocerite applications, therapeutic gymnastics for the development of fingers were prescribed. 25 days after the operation, the finger remained deformed and immobile, but due to the movement of the wrist, the patient retained the opposition function, which allowed him to continue working in his specialty.
Conclusions. The following general principles underlie the treatment of pandactylitis: the process must be limited to the use of antibiotics and enzymes, necrotic tissues removed, and drainage provided. Repeated operations for the purpose of sequestrotomy, tendoectomy are possible. As the inflammatory process decreases, it is possible to reduce the immobilization of the limb and increase the range of motion of the hand.
Share:






Add a comment