Inverted nipple is a developmental anomaly of the mammary glands that affects 10% of women worldwide. Antoine Paraskevas and Ibaa Sabry presented a simple surgical technique for correcting an inverted nipple, which allows you to effectively and quickly get rid of this undesirable phenomenon.
 Dr. Antoine Paraskevas
Dr. Antoine Paraskevas
plastic surgeon,
Member of the French Plastic Association
and Aesthetic Surgery (SOF.CPRE),
author of numerous scientific publications,
scientific director of international congresses
Aesthetic and Plastic Surgery
The essence of the pathology
Inverted nipple is a relatively common special condition characterized by short lactiferous ducts, periductal fibrosis, and insufficient soft tissue under the base of the nipple. This pathology can be congenital or acquired and occurs in about 10% of the female population [1]. Congenital inverted nipples are more common than acquired ones.
Nipple deformity can be caused by a breast infection, carcinoma, breast surgery, or macromastia [2,3]. Inverted nipples can cause certain physiological problems, as well as difficulties with breastfeeding and hygiene. Improper breast hygiene can lead to repeated inflammation of the nipple [2].
There are a number of techniques to correct an inverted nipple. Most of the techniques described in the literature involve the use of sutures, cartilage or tendon grafts, a commercial vacuum system, custom-made disposable syringes, or even piercings to prevent the tendency to retract the nipple [2,4]. We present a simple and very effective surgical technique that minimizes the risk of recurrence of a nipple defect.
Patients and Methods
We treated 13 patients with congenital inverted nipples (24 nipples); 11 patients had bilateral nipple inversion and two had unilateral inversion. In accordance with the classification of Khan and Kong [5], 13 nipples were retracted to the 1st degree, 6 - to the 2nd degree, 5 - to the 3rd degree. Postoperative follow-up of patients lasted from one to three years.
Surgical technique
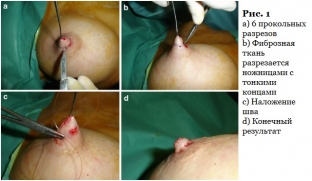
The nipple is pulled out with a skin hook, the procedure is performed under local anesthesia. The surgeon makes six small incisions with a #11 scalpel blade at 12, 2, 4, 8, and 10 o'clock (Fig. 1a). Using fine scissors, we cut the fibrous tissue under the nipple to pull it out. The tips of the scissors are directed down the center of the nipple in order to save a significant amount of tissue under the nipple, which will later serve to hold the nipple in the desired position; in addition, this technique allows not to affect the lactiferous ducts (Fig. 1b). Then, a purse-string suture with polydioxanone 3/0 (PDO) is performed through the above incisions. The purse-string suture is needed to close the so-called dead space area under the nipple and ensure the desired position of the nipple (Fig. 1c). Small incisions are sutured with Vicryl Rapid 6/0 (Fig. 1d).
3 (Fig. 2). A hole is made in the center of the pad, and using a 2/0 silk ligature, we sew the tip of the nipple to the upper borders of the elastic pad. The height of the elastic pad helps keep the nipple in position. The support pad must be worn for 2 weeks, during which time fibrous tissue will form under the elongated nipple (Fig. 3). Bandaging after surgery is not required; Patients can take a shower with an overlay.


Results
No infection, bruising, or nipple necrosis was reported in the immediate postoperative period. Mild pain can be controlled by taking paracetamol orally for 48 hours. During the immediate postoperative period, there may be a temporary sensory impairment of the nipples (reduced or increased sensitivity), which disappears after 3-6 months.During the follow-up period (which lasts from one to three years), we encountered only one case of recurrence of unilateral nipple deformity in a patient who refused to wear a support pad due to summer vacation. The nipple returned to its original deformed position 1 month after the procedure, which was successfully corrected during the second operation using a support pad. With this technique, we gave the nipple a natural look and a very good position, which was maintained throughout the follow-up period (Fig. 4).

Talk
An inverted nipple can cause functional problems, including irritation, inflammation, feeding difficulties, and aesthetic problems [2].Degrees of inverted nipples are defined according to the classification of Han and Hong [5].
There are three degrees of inverted nipples:
- 1 degree - minimal or no fibrosis under the nipple, the nipple can be easily pulled out, and it will remain in this position;
- 2 degree - the nipples are characterized by moderate fibrosis, they can also be pulled out with some effort, but after that they return to their original position;
- 3 degree - nipples have significant fibrosis and can be pulled out with great difficulty, but then quickly return to their original state.
There are two primary goals for corrective surgical procedures:
- sufficient release of fibers and milky ways;
- nipple defect filling [2].
Ritz et al. [4] have described their own simple technique for correcting an inverted nipple, but after such surgery, there is a decrease in lactation. And our technique, which involves incision with scissors pointing down the center of the nipple, allows you to leave the milk ducts intact.
Our quick and simple technique ensures minimal areolar scarring after surgery. In addition, this procedure is performed under local anesthesia. This procedure is effective for the treatment of simple and complex cases of inverted nipples. The use of a support pad is very important as it allows time for healing and prevents the recurrence of fibrosis. We recommend using long-absorbable monofilament suture (we use polydioxanone) or, in severe cases, non-absorbable monofilament suture to keep the nipple in a convex position.
Literature:
- Persichetti P, Poccia I, Pallara T, DelleFemmine PF, Marangi GF (2011) A new simple technique to correct nipple inversion using 2 VY advancement flaps. Ann PlastSurg 67(4):343–345
- Min KH, Park SS, Heo CY, Min KW (2010) Scar-free technique for inverted-nipple correction.AesthPlastSurg 34(1):116–119
- Schwager RG, Smith JW, Gray GF, Goulian D Jr (1974) Inversion of the human female nipple, with a simple method of treatment. PlastReconstrSurg 54(5):564–569
- Ritz M, Silfen R, Morgan D, Southwick G (2005) Simple technique for inverted nipple correction. AesthPlastSurg 29(1):24–27
- Han S, Hong YG (1999) The inverted nipple: its grading and surgical correction. PlastReconstrSurg 104(2):389–395, discussion 396–7
- Burm JS, Kim YW (2007) Correction of inverted nipples by strong suspension with areolar-based dermal flaps. PlastReconstrSurg 120:1483–1486
- Huang WC (2003) A new method for correction of inverted nipple with three periductaldermofibrous flaps. AesthPlastSurg 37:301–304
Plastic surgery today has reached such a level that allows specialists to literally sculpt the desired contour of the face and body. VIPS - Virtual Plastic Surgery - a new direction in plastic surgery, born on the verge of art and 3D technologies:
Share:






Add a comment