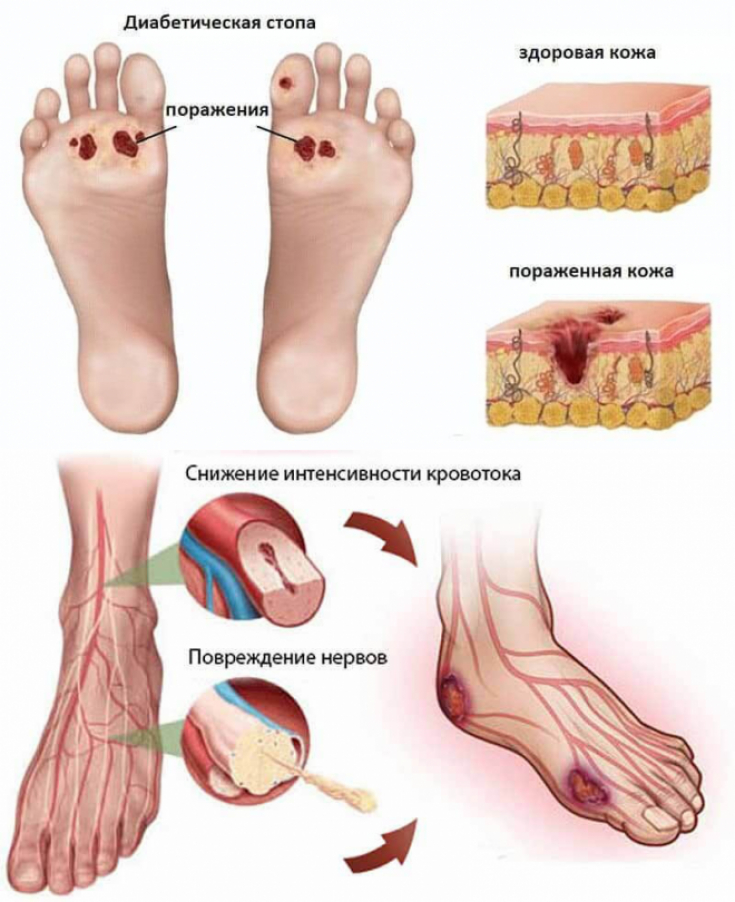
Diabetes mellitus − is a metabolic disorder characterized by hyperglycemia, which results from impaired secretion or sensitivity of body tissues to insulin. Foot ulcer in diabetes mellitus − an open wound that occurs in about 15% of patients and is usually located on the plantar surface of the foot. A foot ulcer is a complication of uncontrolled diabetes mellitus and a symptom of the diabetic foot.
Find out in the article on estet-portal.com how to increase the effectiveness of antibiotic therapy and what are the criteria for choosing a drug for the treatment of foot ulcers as a complication of diabetes.
- Danger of Foot Ulcers in Diabetes Mellitus
- Specific features of diagnosing trophic foot ulcer in diabetes mellitus
- Classification of foot lesions in diabetes mellitus
- Examination of pathogens in foot lesions before antibiotic therapy
- Susceptibility testing before antibiotic therapy improves quality of care
Danger of Foot Ulcers in Diabetes Mellitus
Diabetic foot ulcer increases mortality and is responsible for two-thirds of all non-traumatic amputations worldwide, thereby compromising the quality of life of patients. Knowing the microbial composition of ulcers can improve patient care and treatment.
Follow us on Instagram!
Diabetic foot ulcer has a polymicrobial etiology that includes both aerobic and anaerobic microorganisms. Many researchers note the presence of mixed infection in foot ulcers. Some of the aerobic bacteria associated with diabetes mellitus ulcers include: Staphylococcus aureus, S. saprophyticus, S. epididermis, Streptococcus pyogenes, S. mutans, Pseudomonas aeruginosa, Bacillus subtilis, genus Proteus, Escherichia coli, and Klebsiella pneumoniae. Anaerobic bacteria are represented most often by the species Peptostreptococcus, Anaerobic streptococci, Bacteroides fragilis and Clostridium.
Nondiabetes insipidus: features of diagnosis and therapy
Specific features of diagnosing trophic foot ulcer in diabetes mellitus
Diagnosis of foot ulcers in diabetes mellitus is based on a combination of signs such as erythema around the lesion, local pain and skin temperature increase, the presence of pus, edema and thickening of tissues.
to achieve complete remission.
Risk factors are: middle or advanced age, diabetic neuropathy, infections, smoking, poor glycemic control, leg ulcers or previous amputations, ischemia of small and large blood vessels.
Diabetic foot infection can be superficial or deep. Deep infection affects muscles, bones, superficial fascia of the lower extremity, joints and has various manifestations − from cellulite to wet gangrene. If the foot ulcer in diabetes mellitus progresses to the last stage, the patient is offered treatment in the form of amputation.

Classification of foot lesions in diabetes mellitus
Classification of the severity of diabetic foot depends on the severity of the clinical picture:
- I degree − without objective and subjective symptoms of infection;
- II degree − ulcers have the appearance of lesions on the skin without systemic inflammation and without deep tissue involvement, but with the presence of any two signs: erythema > 0.5-2 cm around the ulcer, local tissue thickening, swelling, soreness, skin temperature increase, pain or purulent discharge;
- III degree− ulcers have the following symptoms: erythema> 2.0 cm with an infection that invades deep structures, has evidence of osteomyelitis, septic arthritis, or a deep abscess;
- IV degree − ulcers are accompanied by a systemic inflammatory response, meet at least two of the following signs: body temperature > 38° C, pulse> 90 beats / min, PaCO2 <32 mmHg Art., leukocytes > 12000/µl or <4000/µl or ≥10% immature.
Osteoarthritis as a complication of diabetes
In a study conducted in Kolkata, India, scientists reported that grade IV ulcers in diabetic patients are commonly infected with two or more bacteria, including ESBL (extended-spectrum beta-lactamases producing - beta-lactamases producing - beta-lactamases extended spectrum), Klebsiella , Staphylococcus aureus (MRSA - Methicillin-resistant Staphylococcus aureus - methicillin-resistant Staphylococcus aureus), etc.
Examination of pathogens in foot lesions before antibiotic therapy
Scientists conducted studies to characterize the aerobic bacteria associated with foot ulcers in diabetes mellitus and to determine drug susceptibility before antibiotic therapy.
The antibiotics studied were erythromycin −15 µg, ceftazidime − 30 µg, ceftriaxone − 30 µg, combination of amoxicillin and clavulanic acid − 30 µg, ofloxacin − 5 µg, levofloxacin − 5 µg, gentamicin − 10 µg, ampicillin − 10 µg combination of sulfamethoxazole and trimethoprim − 25 mcg.
Therapeutic Strategies for the Development of Insulin Analogs
Gram-positive bacteria showed high sensitivity to erythromycin (67.7%) and the combination of amoxicillin with clavulanic acid. (61.2%). Gram-negative bacteria were sensitive to ciprofloxacin (80.4-100%), cefuroxime (25.0-66.7%) and amoxicillin with clavulanic acid (50.0-64.7%). In studies of antibiotic therapy of foot lesions in diabetes mellitus, high resistance to ampicillin (76.5-84.6%), sulfamethoxazole and trimethoprim (41.2-84.6%), as well as gentamicin (58.3-75.0%) was found. ).

Susceptibility testing before antibiotic therapy improves quality of care
The results of a clinical study show that the most common foot ulcer bacteria in diabetes mellitus were Staphylococcus aureus (32.9%), the least common − Klebsiella pneumoniae (20.4%). Women had more infections (62.9%) than men (37.1). Erythromycin was the most effective antibiotic (65.6%) against S. aureus, while Gram-negative bacteria were more sensitive to amoxicillin + clavulanic acid (87.5%) and ciprofloxacin (75.0%).
Advanced Treatments for Diabetes Mellitus
The study recorded 100% of infectious lesions of foot ulcers in patients with diabetes mellitus. Infectious skin lesions were monomicrobial and polymicrobial, and therefore need to be monitored before antibiotic therapy. This study also showed predominance of Gram-negative bacteria.
Thus, for the treatment of diabetic patients with necrotizing ulcers of the foot, it is very important to test for sensitivity to antibiotics before starting antibiotic therapy.
Neuropathic ulcer as a complication of diabetes
Share:






Add a comment