Ptosis of the eyebrows is one of the most common reasons patients seek plastic surgery, as this type of gravitational sagging of the facial tissues is considered the clearest sign of incipient aging. Clinical observations show that gravitational drooping of the eyebrow and ptosis of the eyebrow on one or both sides is a fairly common phenomenon and occurs in both the elderly and young people.
Causes of ptosis
The appearance of early signs of aging in young patients may be due to congenital or acquired hyperelasticity of the connective tissue. In addition, unilateral or bilateral brow ptosis is noted in patients with damage to the frontal branch of the facial nerve. Often, the low position of the eyebrows is asymmetric and is more pronounced on the half of the face where muscle tone is reduced, in the form of smoothing of the nasolabial fold, drooping of the corner of the mouth, lagging behind half of the lip when smiling or talking, and more sluggish facial expressions. Most often, this asymmetry is not associated with the disease and is a physiological feature of the patient, so it may remain invisible to him for a long time.
It should be noted that there are no standards for brow length, width, configuration and position, but most patients prefer to have high or raised brows, brows "house" or "take-off". This preference is shared by many plastic surgeons, especially when the situation requires correction of pseudoblepharochalasis.
The low position or ptosis of the eyebrow is characterized by the following symptom complex: the position of the entire eyebrow or its outer part below the upper edge of the orbit, a decrease in the distance from the lower edge of the eyebrow to the upper ciliary edge, relaxation of the soft tissues of the upper third of the face. The causes of relaxation or decreased turgor of the soft tissues of the frontal and temporal regions are most often morphofunctional changes characteristic of age-related atrophy, which manifest themselves as deep horizontal wrinkles and furrows on the skin of the forehead. These signs of aging are laid in a perpendicular direction with respect to muscle contraction and come in varying degrees of severity.

Determining the position of the eyebrows in ptosis
The most common way to determine the position of the eyebrow is to visually assess this anatomical formation in relation to the upper edge of the orbit. The normal position of the eyebrow is considered when its lower edge is located above the upper edge of the orbit. If the lower edge of the eyebrow is at the level of the upper edge of the orbit, then this indicates its low position or omission, and if the lower edge of the eyebrow is located below the upper edge of the orbit, this is a sign of eyebrow ptosis. Often there are situations when the body of the eyebrow occupies a normal position, i.e. located above or along the edge of the bony orbit, and the outer edge of the eyebrow is lowered. This clinical picture is typical for ptosis of the outer edge ("tail") of the eyebrow. As a rule, such an eyebrow resembles a straight line and does not have an upward bend.
Techniques of operations for the correction of eyebrow ptosis
Recently, surgical techniques with the use of endoscopic equipment have been widely used, which allows the surgeon through small incisions under the control of vision to carry out a sufficiently wide tissue detachment for further movement and fixation in the desired position. Apparently, for these reasons, modern endoscopy is gradually replacing the conventional methods of browpexy in cases where the patient does not have significant relaxation of the soft tissues of the upper third of the face.
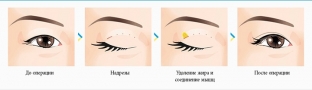
Surgical correction of ptosis of the outer edge of the eyebrow with access through the upper eyelid is a fairly effective and simple method that does not leave additional scars above the eyebrows and does not require special equipment. Usually this stage is performed after upper blepharoplasty, using access through the upper eyelid. For this, soft tissue detachment is carried out under the circular muscle of the eye upward towards the eyebrow. In the projection of the outer half of the eyebrow, the deep fascia venter frontalis m is cut off. occipitofrontalis from the periosteum. Then the soft tissues are exfoliated under this muscle along the periosteum to the middle of the height of the forehead or slightly higher. Detachment is performed stupidly from the outer edge of the eyebrow to its middle, taking into account the exit of the branches of the supraorbital and supratrochlear nerves. Such an area of detachment contributes to a better spreading of the skin near the eyebrow and contributes to the formation of a sufficiently strong scar that holds the outer part of the eyebrow in a higher position. After moving the eyebrow upward, it is fixed at the highest point in the desired position with an external U-shaped or internal suture to the periosteum with synthetic monofilament 2-0 or 6-0, respectively. An external suture is applied through the skin, capturing the muscle (venter frontalis m. occipitofrontalis) and the periosteum. Hemostasis during the operation is carried out using electrocoagulation of bleeding vessels. The wound of the upper eyelid is sutured intradermally with synthetic monofilament 5-0 or 6-0. If necessary, a similar operation is performed on the other side. The sutures on the eyelids are removed on the 4th day, and the U-shaped seam above the eyebrow - on the 10th-12th day.
It should be noted that the correction of brow ptosis in patients with severe relaxation of the soft tissues of the upper third of the face is not effective without eliminating their excess, therefore, in these cases, it is advisable to use surgical techniques with extensive tissue detachment to create their mobility using endoscopic techniques or in the form classical lifting of the soft tissues of the forehead by coronal access. In the latter case, the location of the skin incision should be determined in accordance with the proportions of the face.
Analysis of long-term results from 1 to 3 years showed the high efficiency of a differentiated approach to the surgical correction of eyelid ptosis, since all patients were satisfied with the result of the operation. Based on the analysis of postoperative results, the components of a successful browpexy were identified: a comprehensive assessment of the state of the tissues of the upper and middle thirds of the face and the use of optimally effective surgical techniques in each specific case.
Undoubtedly, browpexy is the operation of choice for the patient, and its positive effects are obvious: the absence of an overhanging crease in the upper eyelid area, an "open" look, a beautiful shape and high position of the eyebrow, a "smooth" forehead with straightened transverse wrinkles.
According to the site rmj.ru
Eyes are a whole world, a reflection of the soul, a mirror of emotions and passions. A wide-open look attracts attention, causes warm smiles and a friendly response from others. We offer you some difficult questions about blepharoplasty, which were answered by one of the leading experts in this field of aesthetic surgery - David Rubenovich Grishkyan:
Share:






Add a comment