
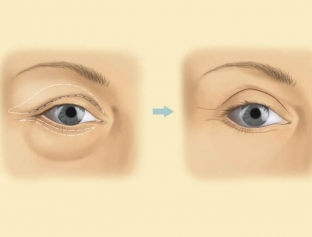
The main goal of any surgical intervention in aesthetic surgery is the correction of defects that distort the appearance of a person, including age-related changes. The aging processes on the face are clearly reflected, first of all, in the eye area. Delicate and thin skin, which is easily affected by various factors, such as mechanical damage and age-related gravitational changes, begins to lose its properties quite early and succumb to various changes. Omission of the crease of the eyelid – one of the earliest signs of this process. What methods of surgical modeling of the eyelid fold are used today – read on estet-portal.com.
Methods for correcting the palpebral fold of the eyelid
The relief of the upper eyelid has a special shape due to the upper orbito-palpebral sulcus and the fold of the eyelid, which is represented by two elements: overhanging and retracted by duplications of the skin. Such a seemingly small structure is formed by many components: eyelid skin, eyelid orbicularis muscle, levator muscle, connective tissue layers, tarso-orbital fascia and orbital fat.
The main part that forms the crease of the eyelid is the fan of distal fibers of the levator aponeurosis, woven into the skin of the eyelid.
All this must be taken into account during the surgical modeling of the palpebral fold of the eyelid.
Crinkle:
- features of the kinematics of the palpebral fold of the eyelid;
- mechanisms of changes in the palpebral fold of the eyelid;
- surgical modeling of the palpebral fold of the eyelid.
Peculiarities of the kinematics of the palpebral fold of the eyelid
Due to the dispersion of the aponeurosis fibers that are woven into the skin and the gradient distribution of forces on them, the eyelid fold lends itself well to the action of the levator, pulling up and completely smoothing out when it is relaxed. The palpebral fold of the eyelid reacts very actively to eye movements:
- if the eye looks up – the crease of the eyelid deepens, lengthens, the eyelashes rise and the crease becomes clear;
- when looking down – the crease almost completely disappears, and the eyelid becomes smooth;
- with an excited look – palpebral fold is pronounced;
- with a faded look – the crease is loosened and the lashes are lowered.
Mechanisms of changes in the palpebral fold of the eyelid
The anatomical structures present in the eyelid area are involved in varying degrees in formation of the palpebral fold.
The features of the formation of the fold depend on the constitution of a person, age-related changes in his body, injuries and diseases that affect morphology.
The folded relief of the skin under the crease of the eyelid is due to excess skin in the area of attachment of the distal fibers of the levator aponeurosis. Massive eyelid occurs as a result of hypertrophic development of the subcutaneous and suborbicular layers with a thickening of loose connective tissue and inclusions of adipose tissue. If a patient has congenital or acquired levator paresis – due to the lack of force applied to the place of attachment, the depth of the fold of the eyelid decreases. The fold is shifted down by fatty hernias of the eyelids and hypertrophy of the orbital tissue.
Surgical modeling of the palpebral fold of the eyelid
Each of the stages of surgical modeling of the palpebral fold of the eyelid has its own important features:
- cutting: it is most convenient to cut along the line of the intended fold;
- skin: resection of the skin is performed in case of its excess and transplantation of a free flap - in case of its deficiency;
- layers of loose connective tissue: the excess layer in front and behind the orbicularis muscle makes the palpebral fold heavier, so it needs to be thinned. The lack of a loose layer is compensated with the help of fillers or orbital tissue;
- circular muscle: resected in cases where there is an excess of it in thickness and area, a decrease in tone, or there are no high fibers of the levator aponeurosis, woven into the skin. The resection area must be above the crease line;
- levator aponeurosis: to reduce the high fold, its upper fibers are cut, to form a high fold – the tarso-orbital fascia is dissected from the aponeurosis and the fold is fixed at the desired height;
- fixation of the crease of the eyelid – this is the main element of surgery. In the standard version, dermal-aponeurotic fixation is performed with U-shaped sutures through the mobilized circular muscle. If necessary, suturing is supplemented by deep fixation and an increase in the number of sutures.
Share:






Add a comment