

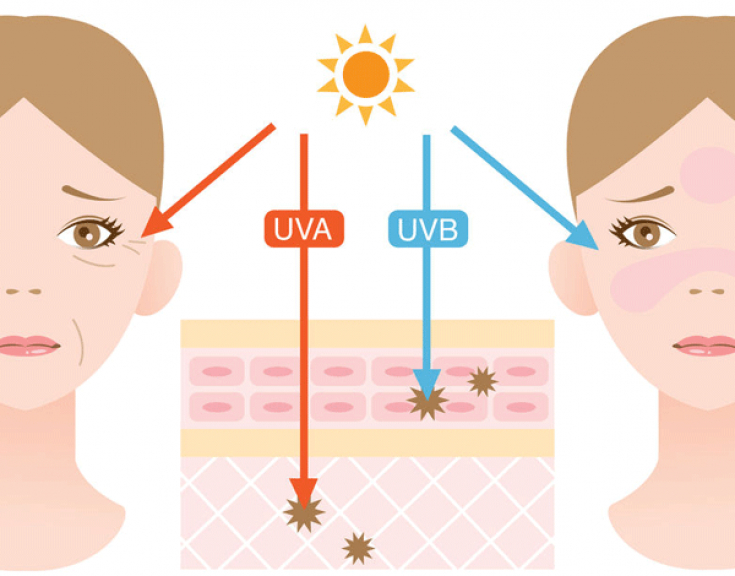
Sun protection at any age reduces the risk of actinic keratosis, squamous cell carcinoma and the progression of photoaging.
Required protection strategies include the wearing of hats and clothing. There are also many sunscreens available that block UV radiation. The value of the sun protection factor (SPF) is equal to the ratio of doses of ultraviolet radiation (predominantly UVB radiation) that lead to erythema (sunburn) with protection to doses that lead to erythema without protection.
UVA blocking by opaque sunscreens, including those claimed to block UVA radiation, cannot be quantified and is usually less than SPF 3. Opaque sunscreens, which often contain titanium dioxide, can provide good UVA protection, but may be cosmetically unacceptable.
In the article estet-portal.com you can get acquainted in detail with the latest and most effective methods of photoaging prevention.
Strategy #1: Peremptory Sun Protection
Applying 170g of sunscreen will provide a total of 5 applications for the entire body of an adult. Daily use is essential for good protection. Sweating and swimming require reapplication.
People usually apply sunscreen thinly and less often than recommended, which significantly reduces protection.
In animals, the use of sunscreen has repaired pre-existing damage. In a randomized human trial, the use of sunscreen with SPF 29 for two years stabilized histological changes in the skin.
Follow us on Facebook
SPF 2 corresponds to 50% block, SPF 15 corresponds to 93% block, and SPF 45 corresponds to 98% block. Controlled studies evaluated daily use of sunscreen (SPF 15 or higher). After 4.5 years, the incidence of actinic keratoses was reduced by approximately 40% compared with the group without sunscreen and by 24% compared with the arbitrary use of sunscreen.
Daily use of sunscreen with an SPF of 15 or higher reduced the incidence of squamous cell carcinoma by 25%, but did not reduce the risk of basal cell carcinoma.
Reducing the risk of basal cell carcinoma depends primarily on reducing sun exposure in childhood.
Although true allergic reactions to active ingredients in sunscreens are rare, 17% of people using sunscreen with SPF 15 or higher over a seven-month period experienced irritation, a major barrier to compliance.
Strategy #2: Careful use of hydroxyacids
Many products that contain alpha and beta hydroxy acids are both exfoliating and moisturizing. Hydroxy acids in low concentrations (typically 4-12%) are ubiquitous ingredients in creams and lotions. In high concentrations, these drugs are used as "peels".
The keratolytic and irritant effects of hydroxy acids depend on the specific acid, concentration and pH.
High concentrations of hydroxy acids or lower concentrations in combination with topical retinoids often cause irritation.

Hydroxyacid-treated skin transmits 20% more UV radiation than untreated skin, making it necessary to use sunscreen.
Compared to sunscreens alone or placebo, use of 5% glycolic acid and 8% lactic acid creams for three to five months reduced roughness and patchy pigmentation in two randomized trials, and pallor in one trial, but without significant effects on wrinkles or actinic keratosis.
A combination of hyaluronic and succinic acids to eliminate skin hyperpigmentation
Strategy #3: Retinoids
Two topical retinoids (tretinoin and tazarotene) have been approved by the Food and Drug Administration (FDA) for "smoothing" fine wrinkles and pigmentation in photoaging. In addition, tretinoin reduces roughness and tazarotene is approved for the treatment of lentigo.
In clinical studies typically lasting six months, there was approximately twice the reduction in wrinkles, patchy hyperpigmentation and roughness than in control subjects who used sunscreen and emollients. A reduction in the appearance of fine lines was found.
The incidence of skin irritation with retinoids increases in direct proportion to the concentration.
UVB penetration is increased by 1/3 in skin that has been treated with topical retinoids compared to untreated skin. Therefore, retinoids are unlikely to provide a clinically meaningful benefit without concomitant sun protection.
Strategy #4: Fluorouracil Cream
Actinic keratoses appear as discrete, rough, pink patches and are common in people, especially people over 50 who have other signs of photoaging. In sunny regions, about 25% of detected actinic keratoses spontaneously regress. However, these lesions are precancerous and can transform into squamous cell carcinoma.
Although there is insufficient evidence, it is likely that treatment of actinic keratoses reduces the risk of developing squamous cell carcinoma.
Topical application of liquid nitrogen (cryosurgery) is considered the standard of care. Fluorouracil 5% cream applied twice a day for 3 weeks on areas of the body with actinic keratosis reduces the number of keratoses by about 70% and reduces epidermal roughness associated with photoaging.

The results are similar to those seen with a medium depth chemical peel.
Significant irritation occurs during the period of application of the fluorouracil cream and for about two weeks thereafter. The cream should not be used during pregnancy.
• Photodynamic therapy (topical application of aminolevulinic acid followed (approximately 16 hours later) by exposure to blue light) is probably less effective than cryosurgery or cream fluorouracil.
• Diclofenac, FDA-approved for the treatment of actinic keratosis, less irritating but much less effective — reduces the number of lesions by approximately 16%.
• While the FDA has not approved 5% imiquimod, it appears to be about as effective as a cream fluorouracil.
• Laser ablation of the epidermis has little effect on the incidence of actin keratoses.
Thank you for staying with estet-portal.com. Read other interesting articles in the "Cosmetology" section. You may be interested in Photoaging: all about the dangers of sunlight
Share:





Add a comment