
Correction of age-related changes in the neck remains an urgent problem for plastic surgeons, despite the many established techniques and methods of operations. About how to optimally correct the aging of the neck and prevent possible postoperative complications, he told estet-portal.com in his article
 "Multivariate Assessment and Surgical Approaches to Neck Rejuvenation" Oscar Ramirez - M.D., Plastic Surgeon, Associate Professor at the Schools of Medicine at Johns Hopkins University and the University of Maryland.
"Multivariate Assessment and Surgical Approaches to Neck Rejuvenation" Oscar Ramirez - M.D., Plastic Surgeon, Associate Professor at the Schools of Medicine at Johns Hopkins University and the University of Maryland.
Factors affecting the aging of the neck and their consideration in the surgical correction of this zone
Neck aging is still an actual problem, despite the fact that in recent years many techniques and procedures for correcting this zone have been described. The result of such a correction, which looks good in the early postoperative period, may be accompanied for several weeks or months by irritating induration, skin laxity, contour irregularities due to & nbsp; ptosis of the salivary gland, hypertrophy of the digastric muscle or subplatysmal fat, which was not addressed during the main surgical intervention.
Despite the fact that a large number of surgeons insist on platysma tying, this solution is not always acceptable for patients with thin necks.
Neck aging depends on the following factors:
- skin elasticity,
- Amounts of accumulated superficial and deep fat in the neck area,
- quality and volume of mandibular support,
- degenerative changes in the cervical spine,
- changes in body mass index.
When evaluating the neck, the surface and deep structures must be taken into account, as they are related to the above factors.
The plan for surgical correction will directly depend on the aesthetic and anatomical results of the examination.
Cervicoplasty should not be limited to skin treatment, correction of subcutaneous fat or platysma muscle. It should make changes in the deep structures of the neck: deep cervical fat, digastric muscle and salivary gland.
Assessing the volume and quality of support for the entire mandible should be an integral part of your pre-operative examination.
Suitable surgical maneuvers should be planned based on a mandatory multivariate assessment.
Not all necks are alike. The following factors influence the aesthetic problems of the cervical area:
- age,
- innate elasticity of the skin,
- accumulation of subcutaneous and subplatysmal fat,
- volume and quality of the skeletal support of the mandible from the chin to the angle of the mandible,
- natural height of the cervical spine,
- presence of arthritic changes in the cervical spine affecting its height and curvature,
- body mass index (BMI).
Acquired or congenital anatomical, aesthetic and metabolic factors significantly affect the aging of the neck.
The aging of this zone with a low body mass index and a long, thin neck will differ significantly from that of a patient with a high body mass index, short neck, and weak skeletal support of the mandible. Between these two extremes there is a huge variety of different cases that require an individual approach to adequately treat the patient.
In the first case (low BMI, long, thin neck with normal curve and adequate mandibular support), simple techniques such as the lateral approach cervicofacial lift will work well. In the second case (high BMI, short neck, weak skeletal support), this simple procedure, which is recommended by many surgeons, will at best give a mediocre result, and at worst will more pronounced anatomical problems and associated aesthetic deformities.
This simple analysis explains why the same correction techniques cannot be used for different anatomical and clinical cases.
Patient considerations to consider when planning a neck correction
Obesity is a growing problem in much of the industrialized world. There are over 6 million obese adults in the US alone. This problem is also relevant among children and adolescents. Since 1980, the number of overweight people has doubled among children and tripled among adults (as of 2006). These are the people that plastic surgeons will consider as patients when they reach middle or old age. And this is not to mention those who have already reached middle and old age.
Obesity affects not only the torso, but also a large part of the face and neck. In such patients, subcutaneous fat accumulates not only in the anterior region of the neck, but also in the back. In them, it also accumulates deep on the platysma muscle, unlike people with average weight. Overweight people, like obese people, also have the problem of thick cheeks and double chins. Obesity is a prerequisite to consider when planning surgery.
The protruding anterior part of the digastric muscle is another problem that must be paid attention to when performing cervicoplasty. The cause of this protrusion may be hypertrophy or malposition of the muscle.
I don't know what causes hypertrophy, but malposition of the anterior digastric muscle occurs due to the low position of the hyoid bone. This is seen in patients with obtuse and hard necks, as well as in patients with microgenia.
Ptosis of the salivary gland is another complex problem. It is observed in many patients and complicates the process of creating a normal neck contour during cervicoplasty. Salivary gland ptosis may occur in patients with thin or heavy necks. Preoperatively, this problem is easier to identify in patients with thin necks. In patients with severe necks, the initial and even significant degree of ptosis of the salivary gland is hidden. This can be a trap for an inexperienced surgeon, because if you miss this, you will end up with a dissatisfied patient: he will claim that you did not remove this piece of fatty tissue from him, which is obviously not true. It will not be easy to help such patients, and the correction at this stage is much more difficult.
Degeneration of the cervical spine – this is a gradual contraction of the cervical spine due to arthritic changes or natural compression or herniation of the intervertebral discs. Usually these phenomena are not noted in the etiology of aesthetic problems of the neck in the process of its aging.
Such changes are common for the entire length of the spine, and for the cervical region they are no exception. These changes will shorten the cervical cylinder, which in turn will push the deep neck and lower part of the oral structure into the zone of least resistance, which is the triangle under the lower jaw and between the neck and chin. As a result, the salivary gland, digastric muscle and subplatysmal fat form a hernia in front and behind. The more superficial cervical envelope, skin and platysma muscle will also become more redundant in both the horizontal and vertical dimensions.
The size of the skeletal support of the mandible also influences the aging process of the lower face and neck. Poor chin support, mandibular body and angle affect the displacement of structures of the lower face towards the neck, blunting the depression under the mandible and changing the cervicomental angle to a more obtuse one. This will also result in more prominent prominence of the submandibular structures.
Preoperative planning for surgical correction of neck aging
Detailed and mandatory analysis is essential for good surgical planning. The patient should be consulted on all issues described in the review: describe the amount of superficial and deep cervical fat, the quality of the skeletal support around the chin and lower jaw; explain how thick or thin the cervical cylinder is, what structures protrude, whether ptosis of the salivary gland is present; assess the amount of excess skin, the presence or absence of platysma bands, and the like. Based on these findings, the surgeon makes a suggestion.
You need to emphasize the need to increase the skeletal support and discuss the treatment of deep cervical structures, the specifics of the approach to neck correction. Do you use a side approach or do you additionally apply an anterior one? How will you treat platysma and skin? These are important decisions, as cervicoplasty will not give a good result without proper pelvic support. If the patient has severe deep structures, then the result of standard cervicoplasty postoperatively can be a heavy neck. Since the treatment of salivary gland ptosis is the most difficult and lengthy, patients should have a good understanding of the process and consequences of the approach. Very often, patients make decisions based on economic factors. He or she must understand that there may be residual effects after surgery, including noticeable problems,


Fig.2. Postoperatively, despite improvement at another level, she shows accentuated fullness of the salivary gland.
When you add more complex procedures to a standard cervicofacial lift, it increases the time and cost of the operation. This is partly true if you add chin augmentation and mandibular angle, as well as deep cervicoplasty. In many cases, the components of planned operations must be performed in stages to achieve the best result and prevent the patient from being under anesthesia for a long time. Routine preoperative CV risk assessment, prevention of blood thinning, and control of high blood pressure are performed in all patients.
Required postoperative follow-up of the patient is carried out under the supervision of a certified nurse with experience in plastic surgery.
The time it takes for a patient to recover and return to work depends on the duration of the surgery. It can vary from 1 to 4 weeks.
Cervicoplasty Surgical Technique: Features of Different Approaches
Lateral and anterior approaches
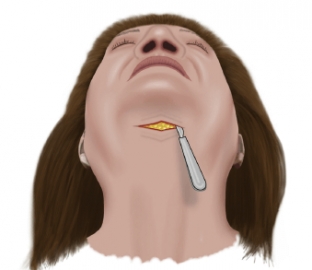
In most patients, lateral and anterior incisions are used. This approach is good regardless of the age of the patient and the amount of work that needs to be done. The reason many patients need work on their front neck is due to platysma, submental fat, etc. I got the best control over these structures thanks to the submental incision. The submental incision is usually made 1.0-1.5cm behind the chin crease. This allows me to draw a subcutaneous direction from this incision to the anterior lower part of the chin and separate the skin junction with the fold under the chin and with the anterior jaw junctions.
This dissection is accompanied by bleeding, and I can control this subcutaneous bleeding to the best of my ability with this approach. This direction allows you to better re-drape the skin. This incision under the chin also allows the platysma to be lifted in the middle and move the skin in the opposite direction. This is usually not possible with a lateral approach only.
Fig.3. The incision under the chin when using the anterior approach is made 1.0 - 1.5 cm behind the crease under the chin.
Obviously there are exceptions when these maneuvers are not necessary and you can handle everything using a side approach.
The lateral approach itself is assigned when there is:
- smooth crease area under the chin,
- lack of chin prominence,
- absence of platysma bands,
- lack of visible premaxillary fossae.
This requires an endoscope, which will allow accurate direction and control of bleeding. Mentopexy and/or chin implants also require an anterior incision.
Cervical fat and cervical bulges
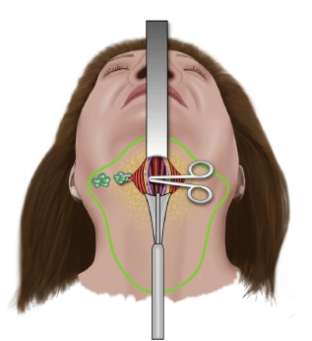
The removal of fat from the neck is done by direct scissor cleansing through the submental approach. I only use liposuction when I'm doing a fully closed approach or reducing the volume of heavy subcutaneous fat deposits and then scissoring good contours.
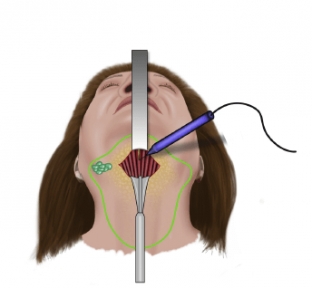
The decision to resect fat under the digastric muscle or under the platysma muscle is made at the time of the operation.Fig.7. On approaching the deep part of the neck, the platysma opens vertically from the anterior point of the protrusion of the chin to the level of the cricoid cartilage.

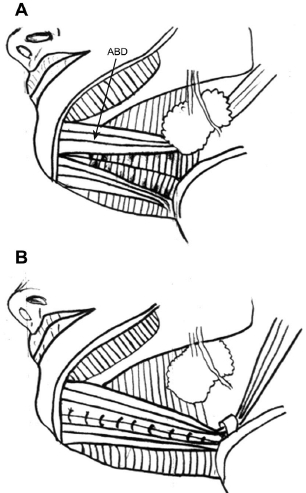
You can predict a high probability of such a performance in the case of a heavy, short neck. After the superficial fat is removed, the neck contour is evaluated. In the case of bulges, the direction is made along the midline, opening the platysma, then a stepwise approach is taken to the subplatysmal structures, starting with deep fat (Fig. 7).
This fat is not limited to the digastric region. It has a trapezoidal shape and runs laterally into the area under the salivary glands (Fig. 8). If you only remove the center section, you will end up with an uneven area under the chin.
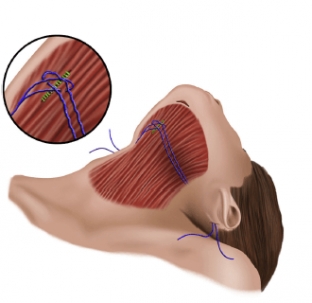
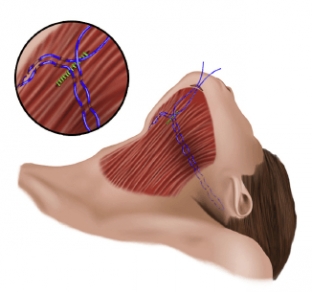
The next step is to assess the contour of the digastric muscle opposite the maxillohyoid muscle. If the digastric muscle is convex, then the first step is to try to raise this muscle in the midline. If it fills the cavity and the contour improves, then we use a corset of inverted sutures
3-0 nylon for the anterior part of the digastric muscle (Fig. 9). If this does not improve the contour, then a tangential removal of the upper layer of the anterior part of the digastric muscle is applied. If ptosis or enlargement of the salivary glands is detected before the operation, or during the operation the glands are convex, then the superficial part of the gland is removed from each side (Fig. 10).
Cervicoplasty
For deep cervicoplasty, we need long and thin instruments. I usually use two lightweight retractors and control bleeding with two small forceps.
- The platysma muscle closes after elevation in the midline.
- If the platysma is thin, I don't remove the excess. I fold it or fold over the edges using knotted stitches.
- In case of platysma bulge, I usually do two Z-plasty on the anterior 4cm of the muscle. I hold the excess muscle tissue with a Ramirez purse-string tissue suture and/or I resect at the very bottom of the dissection area.
- I leave 2 butterfly drains connected to the tubes of the vacuum container, one on each side of the subplatysmal plane and one on each side of the superficial plane. I don't use fibrin glue. I usually remove the drains on the 5-6th day, a little later than the standard of operation usually requires. This helps me prevent possible grayscale.


Note the smooth, clean and well defined neck and the angle between the neck and chin. The patient was approached in both directions. Ramirez's platysmal corset fabric suture was used.


Consequences and complications after cervicoplasty
Complications and consequences of cervicoplasty can range from a simple nuisance to a major problem.
- Involvement of one or more branches of the extreme nerve of the mandible can have dire consequences for the patient. Fortunately, it can be cured in many cases. Nerve repair can be accelerated by electrical myoneural stimulation. To minimize this risk, try to avoid aggressive liposuction and monopolar cautery.
- Acute hematoma in the closed part can become a complication that will threaten the life of the patient. Any hypertension should be under control, and patients should be under constant observation, especially during the first day. During surgery, homeostasis should be checked with a bipolar or coaxial sectional coagulator. Vessels of large and medium size should be fixed with sutures or hemo-clip.
- Subcutaneous/subtissue indurations caused by seromas and hematomas can be treated with a series of injections of diluted trimacinolone. Prevention of seromas involves avoiding hematoma and using a closed system of shallow drains for several days.
- Irregularities of the contour from the accumulation of residual fat can be corrected by liposuction using small cannulas. It can also be prevented by creating a precise outline with sharp scissors.
- Skin necrosis caused by smoking or excessive tension requires re-correction after the area has healed and the skin has softened after a few months. Prevention includes preoperative abstinence from smoking and control of skin tension at the time of wound closure.
- Residual bulge due to hypertrophy of the anterior digastric muscle and/or ptosis of the salivary gland requires a second deep cervicoplasty. Good preoperative evaluation and careful surgical planning are required to avoid these problems.
- Small areas of residual platysma bands can be improved with Botox injections, while larger areas will require revision platysmaplasty. Appropriate surgical technique must be used to avoid residual platysma bands.
Thus, the correction of aesthetic and anatomical deformities of the neck due to the aging process is a complex process, planning and approaches to which depend on the initial examination. Surgical techniques must be tailored to the problems you may encounter. Unlike other parts of the body, in this case a good knowledge of anatomy is a must. Surgery can be very simple or highly technical. Surgeons must have a variety of surgical techniques in their arsenal to ensure the best aesthetic result. Deep cervicoplasty is not superficial cervicoplasty; it's a completely different surgical dimension. Deep cervicoplasty is beyond the power of a conventional facial rejuvenation surgeon. You must be experienced in diagnosing neck problems,
Share:






Add a comment