





Bone-metabolic disorders in chronic kidney disease are a progressive symptom complex that varies with age.
Thus, with a reduced level of diffusible ionized calcium (Ca) in children, a high level of dental caries is observed, and subcompensated form of caries.
For more information on how mineral metabolism is disturbed in chronic kidney disease, and how this affects the condition of tooth enamel, read the article on estet-portal.com.
- Tooth enamel changes in children with chronic kidney disease
- Dental lesions in chronic kidney disease in adults
- Salivary gland studies in patients with chronic kidney diseaseek
Change in tooth enamel with chronic kidney disease in children
For the course of chronic kidney disease in childhood (in cases where CRF was diagnosed before the age of 7), delay in the development of teeth with age is characteristic, but to a lesser extent than bone tissue.
Follow us on Instagram!
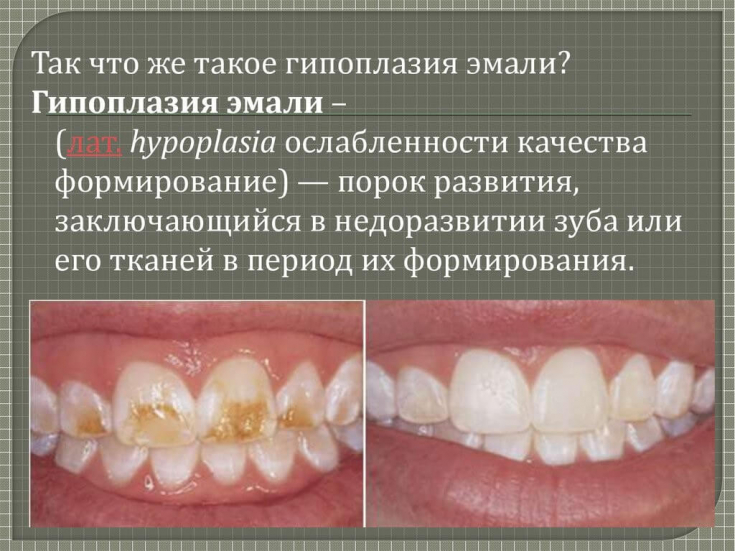
Children show enamel defects, mainly hypoplasia, the location of which is related to the age at which major metabolic changes due to chronic kidney disease appeared.
Children have tooth discoloration, also associated with the severity and duration of CKD.
The rate of formation of microbial plaque is significantly increased in children with chronic renal failure, both for milk and permanent teeth.
Gingival hyperplasia occurs in a certain number of children with chronic renal failure.
The buffer capacity of saliva in children with chronic renal failure is slightly higher than in healthy children, pH, as a rule, is 6.4 (with an average normal of 5.68).
Fixed dentures: why and when are needed
However, the frequency of shedding of Streptococcus mutans and lactobacilli is significantly reduced.
This may be due to increased concentrations of antibacterial substances such as urea in the saliva of children with chronic renal failure.
Dental lesions in adults with chronic kidney disease
In adults with chronic kidney disease, a decrease in bone density as measured by femoral bone densitometry is accompanied by an increase in Ca / P ratios of tooth enamel.
At the backdrop of reducing caries in adults with CKD, the prevalence of non-carious dental lesions.
Patients complain of brittleness and brittleness of teeth.
On examination, increased tooth wear, non-carious lesions (erosions and wedge-shaped defects) are found in 33.3% of cases in people with CKD.
Many authors have found that the concentration of urea, creatinine and phosphorus in the oral fluid of patients with chronic kidney disease increases significantly.
An increase in the concentration of urea and creatinine in saliva leads to an increase in the content of magnesium (Mg) in the enamel of the teeth, which reduces the value of the Ca / P coefficient.
Decrease in residual kidney function, increase in the concentration of urea and inorganic phosphorus in the oral fluid leads to increase in the content of phosphorus (P) in the enamel, which leads to decrease (Ca + Mg + Na) / P coefficient.
In chronic kidney disease of stage 4-5, the electrical conductivity of the enamel increases, that is, demineralization processes occur faster than in healthy people.
Change in the properties of hard tissues of teeth in patients with CKD indicates a change in their morphological and chemical characteristics, which vary from moderate disorders associated with obliteration of the lumen of the dentinal tubules to the widespread formation of dysplastic dentin and thickening of the predentin layer.
Numerous microcracks in the enamel and total sclerosis of the dentinal tubules are also revealed.
In the oral cavity of people with chronic kidney disease, prerequisites are created for the development of carious process:
- poor hygiene;
- high demineralizing activity of the enamel;
- reduction in it Ca / P and (Ca + Mg + Na) / P coefficients.
Despite this, the cariogenic situation does not develop, since the environment in which it is realized acquires an alkaline reaction, which provides protection against caries.
Basic methods for correcting a gingival smile
A characteristic manifestation of the pathology of hard dental tissues in such patients is the high prevalence of non-carious lesionsth.
Salivary gland examination in patients with chronic kidney disease
A study of the salivary glands in patients with CKD led a number of scientists to conclude that their function is impaired due to the harmful effects of urea and creatinine, which is accompanied by:
- decreased secretion;
- increased viscosity of saliva;
- an increase in the rate of calculus formation.
This picture is typical for a subcompensated form of the carious process.
At the background of dysfunction of the salivary glands in people with chronic kidney disease, xerostomia.
What does aesthetic dentistry do
Xerostomia − a subjective sensation of dry mouth, which is relatively common in dialysis patients.
Xerostomia can be caused by a decrease in saliva production secondary to atrophy and fibrosis of the salivary glands due to the use of certain medications, fluid restriction and aging.
Add a comment