

Despite improved clinical guidelines for the diagnosis and treatment of chronic urticaria (HC), there are cases of forms that are resistant to standard line of therapy, in which the patient needs a personalized approach to treatment.
Diagnosis and treatment of chronic urticaria requires:
- a detailed medical history of the patient;
- thorough physical examination;
- carrying out the entire set of routine laboratory tests;
- use a stepwise approach to treatment.
This publication on estet-portal.com provides an algorithm for the treatment of urticaria, taking into account a personalized approach to the treatment of its refractory forms.
- Treatment levels in patients with chronic urticaria
- Main goals of chronic urticaria treatment
- Immunotherapy and treatment of severe forms of chronic urticarias
Treatment levels in patients with chronic urticaria
Modern clinical guidelines based on evidence-based medicine using dose approval of second-generation H1 antihistamines as first-line therapy in patients with chronic urticaria, have entered into a generally accepted consensus regarding such treatment approach.
Atopic Dermatitis Treatment Regimens: Updated Guidelines (Part 2)
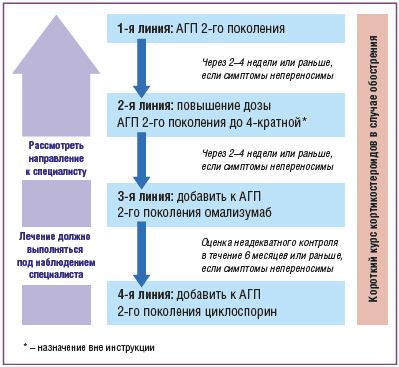
The following levels of therapy are distinguished for patients with urticaria:
- Treatment should be started at a level appropriate to the severity of the disease and the results of previous treatment should be taken into account;
- At each level, an assessment of the tolerability and efficacy of drugs in a given patient should be carried out;
- At any time it is possible to return to the previous level, as soon as control of symptoms of urticarias is achieved.
Follow us on Instagram!
Main goals of chronic urticaria treatment
The goal of treatment for chronic urticaria is to achieve a significant improvement in symptoms with the prevention or reduction of drug side effects.
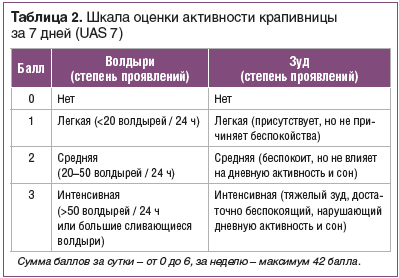
It is important to determine the patient's urticaria activity at baseline and at follow-up visits to the clinic in order to objectively assess response to treatment.
Causes of Toxic Skin Reactions (Part 2)
Activity is scored on the scale UAS (Urticaria Activity Score) − this is a validated gradation that is often used to measure and monitor disease activity in clinical trials for urticaria.
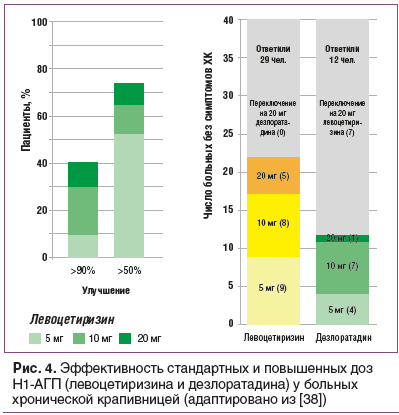
Many patients can respond adequately to standard doses of Hsecond-generation 1-antihistamines, which should be first-line therapyand .
For patients who do not achieve significant clinical improvement, it is recommended to increase the dose of these non-sedating antihistamines to 4 times the recommended dose.
Immunotherapy and treatment of severe forms of chronic urticaria
If dose modulation of first- and second-generation antihistamines does not significantly improve chronic urticaria and/or if the side effects required to achieve this level of clinical improvement are unacceptable, the addition of an immunobiological agent to therapy should be considered >omalizumab, as a second line drug.
If omalizumab cannot be used for a variety of reasons, including cost, or is not well tolerated, consider alternatives:
- cyclosporine;
- dapsone;
- colchicine;
- mycophenolate mofetil;
- sulfasalazine;
- rituximab;
- leukotriene antagonists.
Of these options, evidence-based clinical efficacy is largest for omalizumab and to a lesser extent for cyclosporine A.
The advantages and disadvantages of each of these options should be considered in selecting the appropriate therapy.
Corticosteroids are also effective for chronic urticaria, but their use should be limited to short-term courses for severe flare-ups and should not be used for long-term use as the side effects outweigh their effectiveness.
Causes, risk factors and prevention of diaper dermatitis
Angioedema, isolated , can be treated with 40 mg prednisone for 2 consecutive days and then discontinued without any dose adjustment.
Severeurticarial episodes with or without angioedema can be treated with prednisolone 40 mg/day for 3 days, then tapered by 5 mg daily for 10 days.
Maximum period of glucocorticoid use should not exceed 10 days.How to determine the psychotype of a patient and speak the same language with him
Share:





Add a comment